


I. Introduction
Odontogenic sources have been reported to contribute to approximately 10% of all cases of maxillary sinusitis [1]. Periodontal disease, periapical pathology, unsuccessful endodontic treatment, pulp necrosis, impacted maxillary teeth, and iatrogenic factors such as tooth extraction, implant surgery, and bone grafting in the maxillary sinus can be considered as causative factors for odontogenic maxillary sinusitis [1]. The current incidence is now estimated to be as high as 30% [2]. Furthermore, due to advancements in sinus augmentation techniques and implantology, dental implants is the most common etiology of odontogenic sinusitis [3].
For acute maxillary sinusitis(lasting less than 4 weeks) caused by dental implants, only the causative implant needs to be removed. However, since maxillary sinusitis caused by dental implants is mainly unilateral and progresses chronically(lasting more than 12 weeks), it is necessary to treat not only the causative implant factor but also to manage the obstructed maxillary ostium [4,5]. Therefore, the treatment for dental implant-related maxillary sinusitis involves removing the dental implant and infected bone graft material, and surgically managing the maxillary ostiums [6]. Concomitant endoscopic sinus surgery(ESS) to achieve patency of the maxillary ostium is considered necessary for complete resolution of the disease, prevention of recurrence, and avoidance of complications [7]. Some studies suggest that clinicians should prioritize removing the source of dental infection and only consider ESS if symptoms persist or if complete blockage of the ostium is observed [8]. However, because dental implant-related sinusitis tends to become chronic for more than 12 weeks and the maxillary ostium is frequently blocked, the treatment typically involves ESS. ESS itself is a risky procedure that can lead to fatal complications, such as orbital hemorrhage and cerebrospinal fluid leakage [9]. Moreover, it is a difficult procedure that requires general anesthesia or hospitalization [6].
This study presents case series of patients with chronic maxillary sinusitis caused by dental implants. We aim to propose a novel approach for treatment of dental implant-related chronic maxillary sinusitis in patients with ostium obstruction. This approach involves removing the dental infection and intentionally creating an intentional oroantral fistula(OAF) without the need for ESS. Additionally, this study presents two specific exceptional cases that were not resolved using the method mentioned above.
II. Case Series
1. Patients & Methods
A total of five patients diagnosed with unilateral chronic maxillary sinusitis following dental implant surgery were studied(Table.1). All patients experienced symptoms of maxillary sinusitis, such as postnasal drip(PND), foul odor or pain in the paranasal area for more than 12 weeks following the dental procedure at the time of their initial visit. Furthermore, the Cone-beam CT(CBCT) revealed a general haziness and obstruction of the maxillary ostium in the maxillary sinus on the side where the dental treatment was performed. It was a finding of chronic maxillary sinusitis.
The causative implant or any source of infection related to the implant procedure was removed from all patients. If an OAF existed in the area where the implant was removed, a Penrose drain was placed to maintain the fistula. If there was no OAF, an intentional OAF was formed through intentional perforation. Afterwards, the patient was given oral antibiotics(3rd generation Cephalosporin) and observed. The drain was removed after confirming the patency of the maxillary ostium, which was indicated by 1) symptoms of saline flowing into the nose or throat during drain irrigation, and 2) confirmation of maxillary ostium clearance on CBCT. If either of those two criteria was confirmed, the drain was removed, and the average removal period was 2nd or 3rd postoperative week. After the drain was removed, if the OAF was small, it disappeared naturally. Otherwise, the OAF closure surgery was performed under local anesthesia, at least 4 weeks after the drain removal.
None of the patients treated with the method described above required additional endoscopic sinus surgery to open the maxillary ostium.
2. Case 1
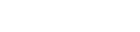
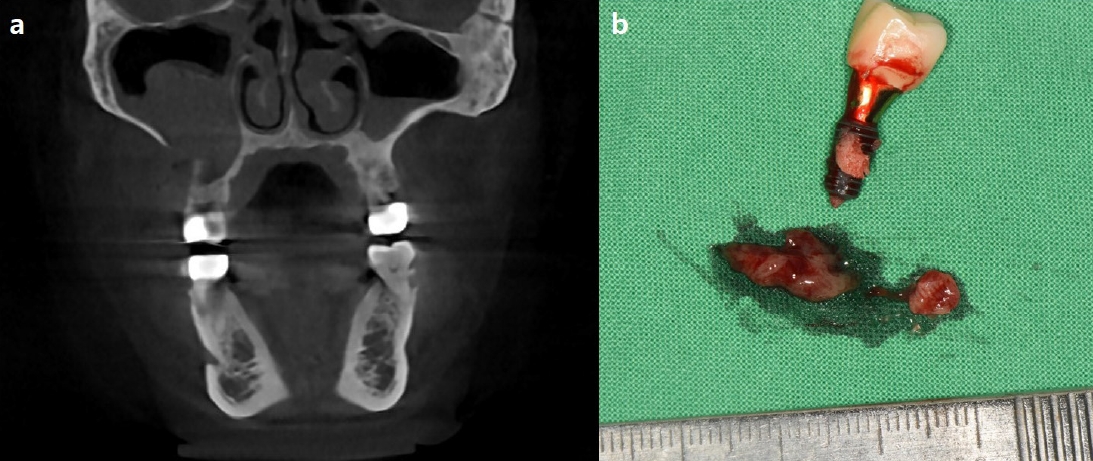
A 63-year-old woman with hepatitis B underwent dental implant placement in the #15 and #17 area, along with a sinus bone graft at a local dental clinic. Right after the surgery, she experienced PND, facial pain, facial swelling, systemic fever, and rhinorrhea. She visited a local Ear-nose-throat(ENT) clinic for a CT scan and antibiotic medication, and was diagnosed as right maxillary sinusitis. Since the symptoms did not subside even after one week of antibiotic therapy, she visited Kyungpook National University Dental Hospital for further evaluation and treatment. According to the CBCT taken on the first day of the visit, the imaging revealed severe mucosal thickening with ostium obstruction(Fig. 1a). The #17 implant was removed using dental forceps, and a 6Fr Penrose drain was inserted to intentionally create an OAF for drainage(Fig. 1b). In the 3rd postoperative week, a follow-up CBCT revealed decreased mucosal thickening and clearance of the blocked ostium(Fig. 1c). Consequently, the drain was removed. Since the oroantral fistula was closed spontaneously and symptoms had also improved, the patient was scheduled for regular follow-up appointments without requiring additional medication therapy.
3. Case 2
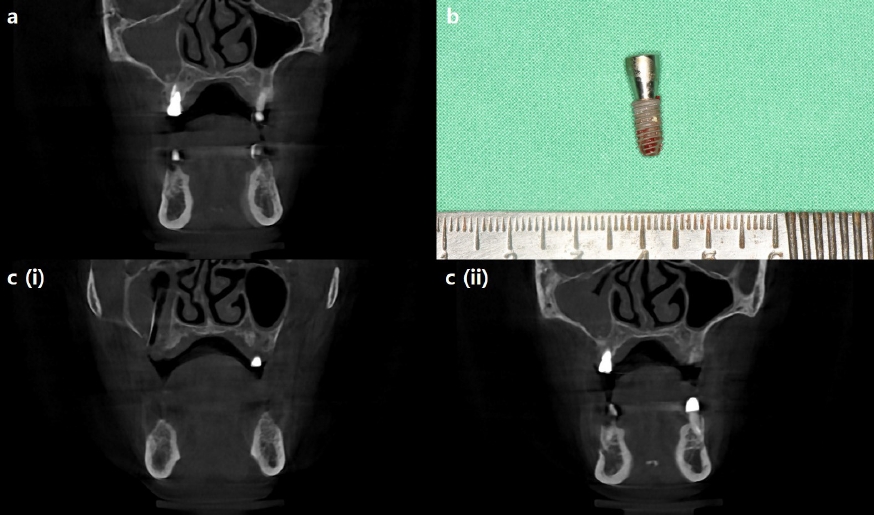
A 72-year-old woman with a history of sinusitis surgery(ESS on right maxillary sinus), hypertension, diabetes, and angina with a history of stent insertion and dual antiplatelet therapy(Aspirin, Clopidogrel), underwent implant placement in the #25~26 area with sinus bone graft at a local dental clinic in 2019. She did not experience any pain or discomfort until May 2022, when she started feeling pain in the #25~26 area, accompanied by systemic fever, swelling, and pus discharge from the gingival sulcus. The pain worsened, so she visited Kyungpook National University Dental Hospital for further evaluation. According to the CBCT taken on the first day of the visit, severe mucosal thickening and complete blockage of the ostium were observed in the left maxillary sinus(Fig. 2a). The #26 implant was removed using dental forceps, and a 6Fr Penrose drain was inserted intentionally to create an OAF for drainage(Fig. 2b). Two weeks after the surgery, a follow-up CBCT was taken, revealing a significant decrease in mucosal thickening and clear ostium patency(Fig. 2c) and the Penrose drain was removed. On the 6th week after the operation, the remaining OAF was closed using a buccal advancement flap under local anesthesia and postoperative CBCT was taken on that day, revealing a further reduction in mucosal thickening(Fig. 2d). According to the CBCT taken on the 6th postoperative month, left maxillary sinus appeared clean and free of inflammation(Fig. 2e), and the patient was then referred back to the local dental clinic for #26 implant placement.
4. Case 3
A 60-year-old man with no prior medical history visited Kyungpook National University Dental Hospital, complaining of PND, stuffy feeling and a foul odor on the right side of his nose. He had implantation surgery for #16, 17 along with sinus augmentation, at a local dental clinic a month before. Two weeks after the implantation, the #16 implant was removed due to persistent mobility issue. After the implant was removed, symptoms of PND, stuffy nose, and a foul odor had begun. Since there was no improvement in symptoms even after taking antibiotics for 5 days at the local ENT clinic, he was referred to Kyungpook National University Dental Hospital for further evaluation and treatment. According to the CBCT taken on the first day of visit, there were severe mucosal pooling in right maxillary sinus and OAF through the #16 extraction socket(Fig. 3a). Based on the severity and invasiveness of maxillary sinusitis, the removal of the #17 implant, sinus curettage, sinus irrigation and insertion of a 6Fr Penrose drain were performed under general anesthesia(Fig. 3b). A postoperative paranasal sinus(PNS) CT was taken on the second day after the surgery, confirming the successful placement of a drain through the right maxillary sinus(Fig. 3c). According to the CBCT taken 2 weeks after the surgery, although the ostium was still blocked with inflamed mucosa, the mucosal thickening had decreased dramatically and the patient showed the sign of ostium patency when irrigating the drain with saline. Therefore, the drain was removed. On the 6th postoperative week, a follow-up PNS CT was taken and ostium patency was finally observed(Fig. 3d). On the 3rd postoperative month, an oroantral fistula in the #16~17 area was closed using a buccal advancement flap under local anesthesia. The stitches were removed a week after, and the mucosa healed favorably.
5. Exception Case 1
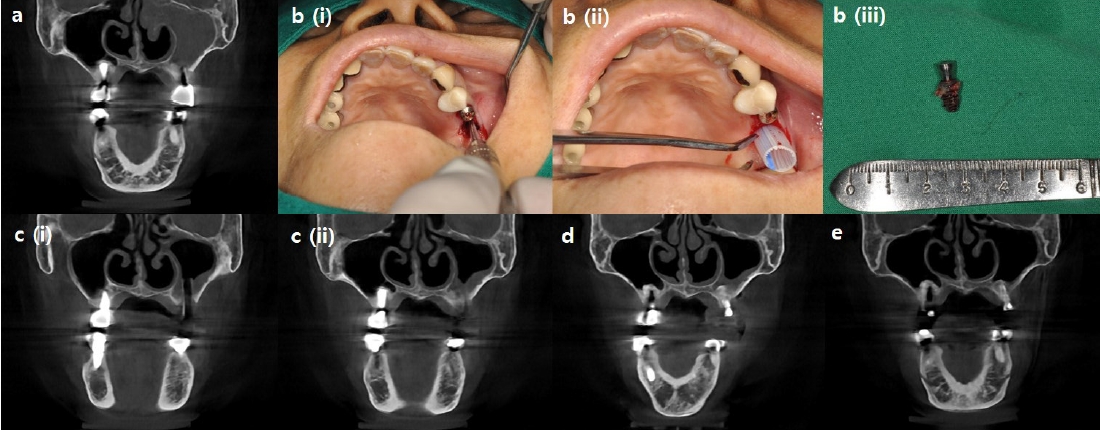
A 63-year-old man with a history of angina and stent insertion was referred from a local dental clinic due to an irregular type of right maxillary sinusitis. He had an implantation surgery on #16 area with sinus bone graft at a local dental clinic in 2022. Pain, swelling and a foul odor began in June 2023. Even after undergoing incision and drainage surgery at the local dental clinic, the symptoms persisted without any improvement. As a result, he visited Kyungpook National University Dental Hospital for further evaluation and treatment. According to the CBCT taken on the first day of the visit, severe mucosal thickening with multiple internal calcifications on right maxillary sinus floor and discontinuity of the lateral wall of right maxillary sinus was observed(Fig. 4a). The initial diagnosis for this imaging was chronic maxillary sinusitis caused by the #16 implant and infected bone graft materials. The #16 implant was removed using dental forceps, and a 6Fr Penrose drain was inserted into the extraction socket to intentionally create an OAF. Granulation tissue from the right maxillary sinus was collected and sent out for biopsy(Fig. 4b). After a week, there were no significant improvements in symptoms, so additional antibiotics were prescribed for another week. The biopsy result came out as “Malignant lymphoma, suspicious for diffuse large B-cell lymphoma.” Subsequently, the drain was removed, and the patient was referred to the hemato-oncology department for additional assessment and chemotherapy.
6. Exception Case 2
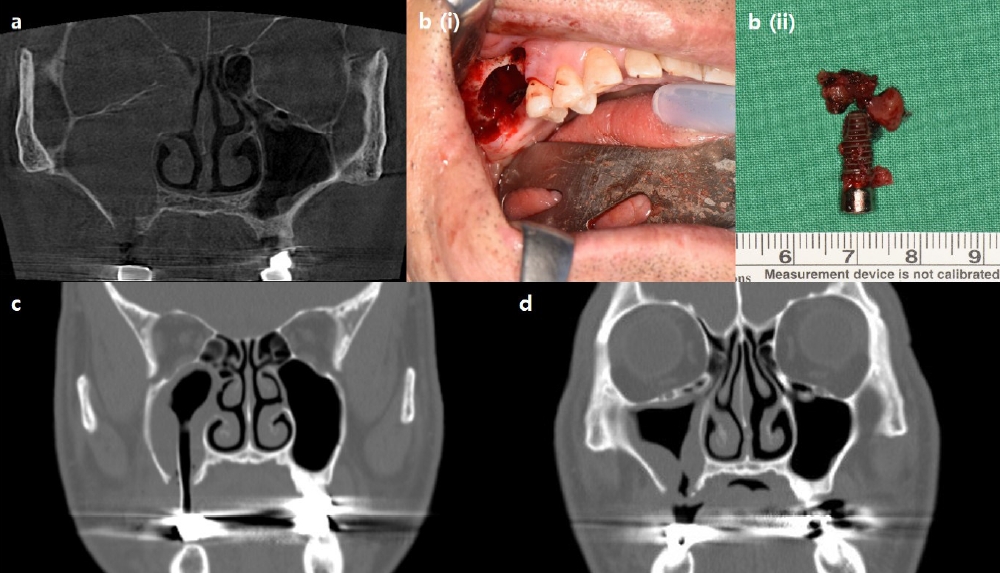
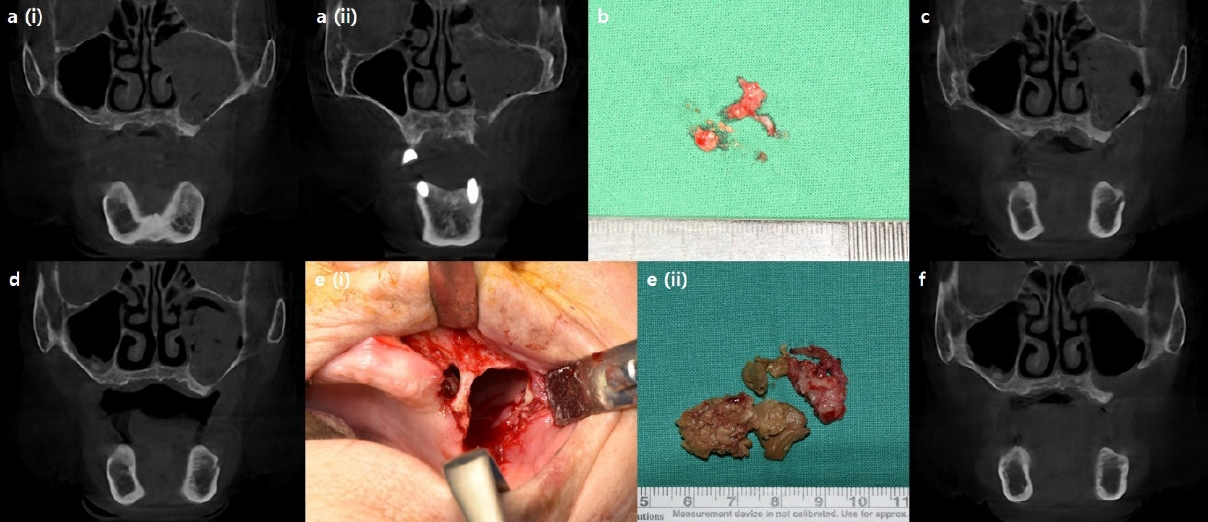
An 84-year-old woman with osteoporosis, hypertention, diabetes, and a history of pacemaker insertion due to AV block visited Kyungpook National University Dental Hospital in October, 2023. She had an implant on left maxillary canine area removed about 6 months ago due to peri-implantitis. In August 2023, a foul odor, pus discharge and discomfort began in the left maxillary canine and premolar area. After a month of systemic antibiotic treatment, her symptoms have improved. However, due to invasive bone destruction and severe mucosal thickening in the left maxillary sinus, she was referred to Kyungpook National University Dental Hospital for further evaluation. According to the CBCT taken on the first day of the visit, the examination revealed destruction of the sinus floor, presence of sequestrum, severe mucosal pooling, and blockage of the ostium in the left maxillary sinus(Fig. 5a). She was initially diagnosed with left maxillary sinusitis with osteomyelitis. After 2 weeks of antibiotics medication, a sequestrectomy, sinus irrigation, and insertion of a 6Fr Penrose drain were performed to intentionally create an OAF under local anesthesia. Inflammatory tissue from the sinus was collected and sent for biopsy(Fig. 5b). The biopsy result later confirmed the presence of osteomyelitis, as anticipated. On the 3rd postoperative week, the patient showed signs of ostium patency when irrigated with saline, so the drain was removed. However, the CBCT did not show any significant improvement in the degree of mucosal thickening, and the ostium was still blocked with thick mucosa containing scattered radiopaque particles, which could indicate the possibility of a fungal infection such as aspergillosis(Fig. 5c). CBCT taken on the 6th postoperative week revealed that the left maxillary sinus was still heavily filled with inflamed, thickened mucosa, and the ostium was also blocked(Fig. 5d). Due to the delayed healing of the sinusitis, a more invasive surgical intervention under general anesthesia was performed, including sequestrectomy, surgical curettage, sinus irrigation, and closure of the OAF using a buccal advancement flap(Fig. 5e). The patient visited for a postoperative check a week after the operation, and the mucosa had healed favorably. The biopsy results confirmed the presence of both aspergillosis and osteomyelitis, as suspected. According to the postoperative CBCT taken one month after the general anesthesia operation, the left maxillary sinus became clean along with the clear ostium, and the patient was referred back to the local dental clinic for additional prosthetic treatment(Fig. 5f).
III. Discussion
Odontogenic maxillary sinusitis is a common subtype of sinusitis, and its incidence rate has been increasing due to the widespread use of dental implants and sinus augmentation techniques [2]. A specific protocol for the management of odontogenic maxillary sinusitis has not yet been established, but its surgical treatment options can be divided into two parts: management of dental infection and sinus surgery for patency of the maxillary ostium [10]. Odontogenic maxillary sinusitis usually presents as chronic maxillary sinusitis of more than 12 weeks duration, usually unilaterally in the maxillary sinus with an odontogenic etiology. Therefore, the treatment should also be performed as a form of treatment for chronic maxillary sinusitis. Numerous studies have supported dental treatment combined with ESS as the most effective approach for achieving complete resolution preventing recurrences in chronic odontogenic maxillary sinusitis [3,6,10]. Some studies have advocated that in cases where there is a clear dental infection source, it is logical to target the infection source first and then perform sinus surgery, such as ESS, as the next step in treatment only if symptoms persist [7]. However, if the osteomeatal complex is obstructed, odontogenic sinusitis does not easily resolve by removal of dental infection alone, and it can be a predictor of indication for ESS [7,11].
Dental implant-related maxillary sinusitis is a type of odontogenic maxillary sinusitis that presents unilaterally and chronically [4]. Causes of maxillary sinusitis following dental implant placement include perforation of the Schneiderian membrane during surgery and the presence of preexisting maxillary sinusitis [12]. Perforation of the Schneiderian membrane leads to dislodgement of bone graft materials and contamination of the exposed implant surface inside the maxillary sinus, resulting in maxillary sinusitis [13]. Therefore, the treatment consists of removal of both the contaminated implant and the bone graft materials [14]. In addition, in chronic cases, the maxillary ostium may become obstructed, and sinus surgery should be performed to open the ostium at the same time [3].
In this case series, the implant was exposed within the maxillary sinus, and despite bone grafting, the bone graft material was not clearly radiographically visible. The contaminated implant was removed, and an OAF was created with the removed portion to relieve pressure within the maxillary sinus and allow for drainage of pus and contaminants. In all patients, when the OAF was created for the first time, there was no evidence of ostium patency or fluid running through the nose when irrigated with the saline. However, after antibiotics administration and dressing, the patients showed signs indicative of the ostium patency. Then, CBCT was taken to confirm radiologic patency of the ostium, and the drain was subsequently removed. Afterwards, the OAF was closed spontaneously, or fistula closure surgery was performed using a buccal advancement flap under local anesthesia.
In the first three cases presented in this study, all of the maxillary sinuses exhibited severe mucosal thickening and obstructed ostium. Instead of referring patients to an ENT specialist for ESS, the dental infection sources were eliminated, and intentional OAFs were created using Penrose drains. In cases 1 and 2, the dental implants, which were the source of infection, were removed through surgical procedures. Penrose drains were then inserted through the surgical sites. In both cases, the drains were removed since dramatic decrease in mucosal thickening was observed, and ostium patency was confirmed three weeks and two weeks after the surgery.
In case 3, however, the patient had already removed one of the dental implants and presented with pre-implant site gingival healing with a fully blocked ostium. Gingival incision and Penrose drain insertion was performed for creation of the intentional OAF. On the 2nd postoperative week, despite the continued obstruction of the ostium, there was a significant decrease in mucosal thickening in the right maxillary sinus, leading to the removal of the Penrose drain. On the 6th postoperative week, cleared ostium patency was finally observed. In this case, although the contaminated implant was removed beforehand, the contaminants in the maxillary sinus were not completely removed, therefore resulting in persistent chronic maxillary sinusitis. This case illustrates that chronic implant maxillary sinusitis requires treatment of the maxillary sinusitis itself as well as removal of the source of contamination.
However, there were two cases in which this method did not show significant improvement in symptoms because of differences between the initial diagnosis and the final diagnosis determined by histopathological examination. In the first exception case, the patient was initially diagnosed with right maxillary sinusitis caused by the #16 implant fixture and bone graft materials. However, the final biopsy result revealed “Malignant lymphoma, suspicious for diffuse large B-cell lymphoma,” and the patient was referred to the hemato-oncology department for chemotherapy. Since diffuse large B-cell lymphoma originating from the maxillary sinus can be misdiagnosed as a benign inflammatory condition, it is important to raise awareness and explore other potential causes if the patient does not show improvement with antibiotics and standard conservative treatments [15]. In the second case, the patient was initially diagnosed with left maxillary sinusitis caused by osteomyelitis. Even after several weeks of drainage through the intentionally created oroantral fistula and antibiotic therapy, the haziness of the maxillary sinus did not seem to decrease. Therefore, other etiologies, such as fungal infections like aspergillosis, were taken into consideration and final biopsy result also confirmed the presence of aspergillosis. Since surgical debridement is the primary treatment for aspergillosis [16], the patient underwent a surgical intervention under general anesthesia and recovered well.
As shown in these cases, when there are no signs of spontaneous ostium patency despite the treatment of chronic maxillary sinusitis as described above, or when the radiopacity of the maxillary sinus does not resolve over a prolonged period of time even if there are clinical signs of ostium patency, causes other than odontogenic origin should be suspected, such as malignancy, hematologic tumor or mycosis.
Although a gold standard for the treatment of dental implant-related chronic maxillary sinusitis has not been established, a combination of infected implant removal and ESS is widely used due to its effectiveness. However, this treatment method requires additional visits to the ENT and possibly general anesthesia and hospitalization for ESS. This study presents three cases in which patient with severe maxillary sinusitis and a blocked ostium was treated without performing ESS. The treatment involved removing the dental infection source and creating an intentional oroantral fistula by inserting a Penrose drain in the maxillary sinus. This study demonstrated that intentional oroantral communication facilitate the drainage of inflammatory tissue and the clearance of ostium obstruction in cases of maxillary sinusitis, with the exception of rare conditions such as malignant tumors or fungal infections. While this method is not universally applicable and has some limitations, it can be considered as one of the treatment options for severe odontogenic maxillary sinusitis. It can help alleviate the patient’s symptoms without the need for additional sinus surgery by an ENT specialist.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



