IgG4-related disease on parotid gland mimicking pleomorphic adenoma: Report of a case
Article information

Abstract
IgG4-related disease (IgG4-RD) is a rare immune-mediated inflammatory disorder that can involve salivary glands and mimic benign tumors radiologically. This report presents a case of IgG4-RD of the parotid gland initially suspected as pleomorphic adenoma. A 66-year-old female patient presented with swelling and pain in the left temporomandibular joint region. Magnetic resonance image and ultrasonography-guided fine needle aspiration suggested a benign cystic tumor, and both parotid lesions were initially suspected to be bilateral pleomorphic adenomas. Excisional biopsy was performed on the larger lesion in the left parotid gland. Histopathological examination revealed a lymphoepithelial cyst with storiform fibrosis and dense infiltration of IgG4-positive plasma cells (72/HPF). Serum IgG4 level was elevated (141 mg/dL), satisfying the diagnostic criteria for IgG4-RD. The patient was referred to rheumatology for systemic evaluation and steroid therapy was considered. This report highlights the diagnostic challenge of differentiating IgG4-RD from benign parotid tumors.
Introduction
Immunoglobulin G4-related disease (IgG4-RD) is a recently recognized fibroinflammatory condition that can affect nearly any organ system, including the pancreas, bile ducts, retroperitoneum, lacrimal glands, and salivary glands [1-3]. First described in the context of autoimmune pancreatitis, the disease has since been classified as a systemic condition characterized by a lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells, storiform fibrosis, and obliterative phlebitis [4].
In the head and neck region, IgG4-RD most frequently involves the major salivary glands and can manifest clinically as painless swelling, which may be mistaken for benign neoplasms such as pleomorphic adenoma or Warthin tumor [4,5]. Among these, pleomorphic adenoma is the most common benign tumor of the parotid gland and typically appears as a well-circumscribed, slow-growing mass on imaging. While pleomorphic adenomas usually require surgical excision, IgG4-RD is often responsive to medical therapy with corticosteroids and immunosuppressants [5]. Radiological findings are often nonspecific and may mimic both neoplastic and infectious processes, rendering clinical diagnosis difficult [6]. While imaging modalities such as ultrasonography and magnetic resonance imaging (MRI) are useful for identifying lesions, they often fail to distinguish IgG4-RD from other massforming diseases [7].
Histopathologic examination remains the gold standard for diagnosis. The diagnostic framework for IgG4-RD has undergone significant evolution to improve clinical specificity. Initially, the 2011 Comprehensive Diagnostic Criteria established the foundational triad of organ enlargement, elevated serum IgG4 levels (>135 mg/dL), and characteristic histopathological findings [8]. This was further refined by the 2012 International Consensus on Pathology, which standardized the histological requirements such as storiform fibrosis and obliterative phlebitis [9]. More recently, the 2019 ACR/EULAR Classification Criteria introduced a weighted scoring system to better distinguish IgG4-RD from its clinical mimics [10].
The 2019 ACR/EULAR classification criteria emphasize the need for histologic triad (dense IgG4+ plasma cell infiltration, storiform fibrosis, and obliterative phlebitis), along with serologic evidence of elevated IgG4 levels, to establish the diagnosis [1,3,4,10].However, awareness and recognition of this disease in the context of parotid gland lesions remain limited, especially when imaging findings strongly resemble benign tumors [5].
Given the therapeutic implications—wherein corticosteroid therapy can often induce rapid remission and prevent unnecessary surgery—accurate and timely diagnosis of IgG4-RD is critical [11]. In this report, we describe a case of parotid IgG4-RD that radiologically mimicked pleomorphic adenoma but was definitively diagnosed through histopathology and immunohistochemistry, reinforcing the importance of tissue confirmation in ambiguous glandular swellings.
Case Report
A 66-year-old female presented to the Department of Oral and Maxillofacial Surgery at Jeonbuk National University Dental Hospital with a chief complaint of swelling and pain in the left temporomandibular joint area. Her past medical history was unremarkable. Upon clinical examination, a mass with a firm, indurated feel was palpated, and a computed tomography (CT) scan was initially performed for an accurate diagnosis (Fig. 1A).

A. Axial computed tomographic image shows contrast enhancement in both parotid glands. B. Axial magnetic resonance image (MRI) image shows contrast enhancement in both parotid glands. C. Coronal MRI image shows contrast enhancement in both parotid glands. A-C. The left and right arrows indicate the lesions on the left and right sides, respectively, showing a difference in size. D. Sagittal MRI image shows contrast enhancement in the left parotid gland.
Subsequent magnetic resonance imaging (MRI) revealed a well-defined, predominantly cystic ovoid mass measuring approximately 2.4 × 1.6 × 2.7 cm in the upper pole of the superficial lobe of the left parotid gland. This lesion exhibited rim enhancement, enhancing internal septum-like structures, and a small amount of internal hemorrhage, suggesting a pleomorphic adenoma. The left parotid lesion was confirmed to be a benignappearing, predominantly cystic mass with a minor solid portion noted inferiorly and no evidence of increased internal vascularity. In the upper pole of the superficial lobe of the contralateral (right) parotid gland, a well-defined ovoid enhancing nodular lesion measuring approximately 7 mm with suspected focal internal cystic changes was identified (Figs. 1B-D). These bilateral lesions were located symmetrically but showed a significant difference in size. Despite this difference in size, an accurate differential diagnosis based solely on these radiographic findings was difficult due to the bilateral presentation. Therefore, fine-needle aspiration (FNA) was planned to evaluate the internal components of the left parotid lesion. Following three passes of FNA, approximately 2 cc of pus-like material was aspirated, which resulted in a slight decrease in the size of the mass to 2.0 × 1.2 × 2.3 cm (Fig. 2). The cytological examination results revealed the detection of a small amount of inflammatory cells, indicating a non-specific benignity.
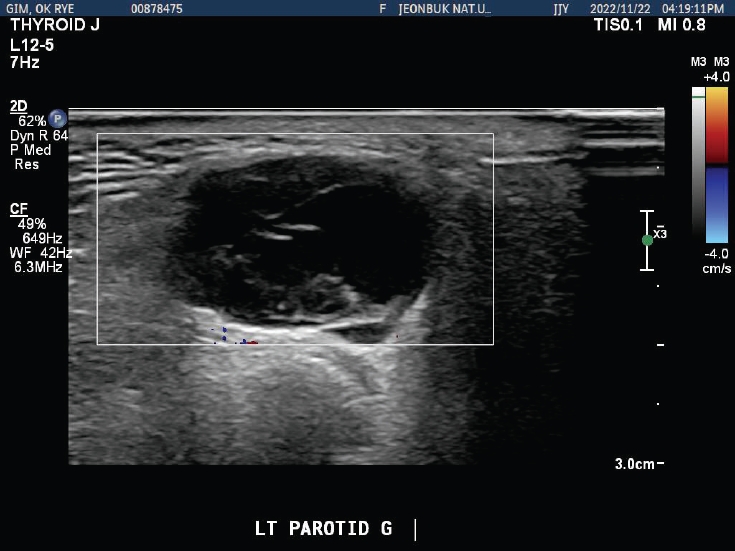
Ultrasonography-guided fine needle aspiration cytology shows benign looking cystic mass.
The patient was scheduled for surgical excision and the procedure was performed as follows. The surgical site was prepared and routinely draped in a doublehead fashion. A marking was made for a pre-auricular approach, followed by an incision through the skin and subcutaneous fat layers. Blunt dissection was meticulously performed through the SMAS layer, ensuring no hemorrhage or vascular injury. Upon exposing the parotid capsule, dissection was carried out using mosquito forceps to reveal the underlying mass. The lesion was then dissected using a combination of mosquito forceps and electrocautery. Notably, the mesio-superior portion of the mass exhibited signs of adhesion to the parotid tissue, necessitating the inclusion of adjacent salivary tissue during dissection; an additional tissue component, appearing as a newly formed tumor, was also identified on the medial aspect. Following the complete excision of the lesion, a permanent biopsy was requested for definitive histopathological diagnosis. Hemostasis was secured with the application of oxidized regenerated cellulose. Finally, the parotid capsule was repositioned, and the surgical site was closed via a systematic layered suture technique to ensure anatomical restoration (Fig. 3).

A. Preoperative design of the incision. An incision line is demarcated in the left preauricular area for the preauricular approach to the parotid gland. B. Intraoperative view of the lesion. The parotid mass is exposed after blunt dissection along the preauricular incision, immediately before the excision. C. Post-excision view. The surgical field is shown after the complete removal of the left parotid mass, with the facial nerve branches carefully preserved. D. The resected specimen
Following the surgical excision, histopathological examination of the resected specimen revealed a lymphoepithelial cyst characterized by extensive fibrosis and dense lymphoplasmacytic infiltration Immunohistochemical staining demonstrated >50 IgG4-positive plasma cells per high-power field (72/HPF), along with obliterative phlebitis and eosinophil infiltration (Fig. 4).

A. White arrows show obliterative phlebitis, black triangles show eosinophils. Findings are consistent with lymphoepithelial cyst with fibrosis (H&E stain, 100um). B. Black triangles show brown stained cells which have IgG4 positive reaction (72 IgG4+ plasma cells/high-power field) (DAB stain, 300um ).
Following these findings, an additional serum test was conducted, which showed IgG4 levels of 141 mg/dL, confirming that the patient met all three diagnostic criteria. Consequently, the patient was definitively diagnosed with IgG4-RD associated with IgG4-positive cellular infiltration. After undergoing surgical resection in the Department of Oral and Maxillofacial Surgery, the patient was transferred to the Department of Rheumatology for further systemic evaluation and management. For the contralateral lesion, a watchful waiting strategy was adopted.
The patient was referred to the Department of Rheumatology, and low-dose steroid therapy was planned for the conservative treatment of the contralateral lesion. Follow-up examinations confirmed an improvement in the patient's condition after taking the corticosteroid agent, micronized deflazacort (3 mg), once daily for approximately two years.
Discussion
This case presents a rare instance in which IgG4-RD of the parotid gland mimicked a pleomorphic adenoma on imaging studies. Both magnetic resonance imaging and ultrasonography-guided fine needle aspiration suggested a benign salivary gland neoplasm, and the possibility of IgG4-RD was not initially considered.
In the present case, the initial surgical intervention was prompted by these deceptive imaging features, which is a recognized diagnostic pitfall [12]. Ultimately, definitive diagnosis was achieved through surgical excision and histopathologic examination, which revealed features consistent with IgG4-RD. Fortunately, the contralateral lesion could be managed conservatively without surgery. The diagnosis of IgG4-RD remains challenging due to its clinical and radiologic mimicry of benign tumors, particularly in the salivary glands. Radiographically, it may appear as a well-circumscribed, cystic mass, making it difficult to distinguish from pleomorphic adenoma or Warthin’s tumor. In our case, the imaging findings were consistent with these features, emphasizing the need for heightened awareness of IgG4-RD in such presentations.
Although most benign salivary gland neoplasms, such as pleomorphic adenoma, typically present as unilateral masses, bilateral occurrence has been documented in rare instances [13]. Due to these established clinical possibilities, the presence of a contralateral lesion in our patient did not initially exclude the suspicion of a benign neoplastic process.
Differential diagnosis based solely on radiographic imaging is challenging. Pleomorphic adenomas typically present as well-circumscribed, slow-growing masses with cystic components, features that can also be seen in IgG4-RD. The diagnostic triad—storiform fibrosis, dense lymphoplasmacytic infiltration, and obliterative phlebitis—is essential in differentiating IgG4-RD from other pathologies [1]. Moreover, an elevated serum IgG4- concentration (>135 mg/dL) and increased IgG4+ plasma cells (>50/HPF in this case) provide strong supportive evidence [1,4]. Thus, imaging studies must be supplemented by histopathological and immunohistochemical analyses for definitive diagnosis. Recent studies have underscored that IgG4-RD is often underdiagnosed in head and neck regions, particularly due to overlapping imaging features with neoplasms [5]. Tissue biopsy with immunohistochemistry remains the gold standard for diagnosis. The standard diagnostic criteria for IgG4-RD require 1) clinical evidence of organ involvement; 2) serum IgG4 level ≥135 mg/dL; and 3) histopathologic features including >10 IgG4-positive plasma cells per HPF and IgG4+/IgG+ plasma cell ratio >40%. Our patient met all three criteria [3,4].
IgG4-related sialadenitis is a systemic fibroinflammatory condition that responds remarkably well to medical therapy, even without surgical resection. In terms of management, IgG4-RD is typically responsive to systemic corticosteroids, which represent the first-line treatment and often induce rapid remission [6,11]. In patients with relapsing or refractory disease, B-cell depletion therapy with rituximab has shown promise as a steroidsparing alternative [4,14]. In our patient, the localized nature of disease and lack of systemic involvement justified a conservative strategy with monitoring of the contralateral lesion. Importantly, this case aligns with literature advocating for multidisciplinary collaboration, especially between rheumatology, pathology, and surgical teams, in managing atypical presentations [4,6]. Treatment generally involves corticosteroids as the first-line therapy. Immunosuppressive agents or rituximab may be considered in refractory cases. Studies have shown that long-term maintenance therapy with low-dose corticosteroids significantly reduces the rate of relapse [15]. In instances of localized disease without functional compromise, surgical resection or close observation may be sufficient. A misdiagnosis can lead to unnecessary surgery or delayed treatment, both of which can be avoided through a comprehensive, collaborative diagnostic approach.
In conclusion, this report highlighted the critical need to consider IgG4-related disease in the differential diagnosis of parotid gland masses, especially when imaging findings suggest pleomorphic adenoma. Although rare, IgG4-RD is a clinically significant condition that can affect salivary glands and other organs. Non-surgical interventions, particularly corticosteroid therapy, are often effective and should be considered as first-line treatment when systemic disease is suspected or confirmed [16].
Notes
Conflicts of Interest
None
Acknowledgement
The authors acknowledge the use of Gemini and Chat GPT for English translation and language editing. All authors have reviewed the final manuscript and assume full responsibility for its content