임플란트 주위염 치료의 최신 지견
Current perspectives on the management of peri-implantitis
Article information

Trans Abstract
Since the introduction of health insurance coverage for dental implants in 2014 for individuals aged 75 and older, the policy has expanded to cover up to two implants for those aged 65 and older. As a result, more than 600,000 health insurance-covered implant procedures are now performed annually at the local clinic. As of December 2024, South Korea has entered a super-aged society—with over 20% of the population aged 65 and older—it is expected that the number of dental implant procedures for the elderly will continue to increase. With the rise in implant procedures, the incidence of peri-implantitis is also growing. Initially described as a condition similar to periodontitis, peri-implantitis has since been systematically defined through ongoing research. At the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions, peri-implantitis was defined as“a pathological condition of dental plaque origin occurring in the tissues surroundings dental implants, characterized by inflammation of the mucosa surrounding the implant and subsequent progressive loss of supporting bone”. In response to this, the Korean Academy of Periodontology published a consensus report in 2024, which outlines a classification system for peri-implantitis based on bleeding on probing, probing depth, and the condition of surrounding alveolar bone. Treatment approaches for peri-implantitis are generally similar to those for periodontitis. Both non-surgical and surgical therapies aim to remove plaque and calculus, control inflammation, and promote reattachment of the peri-implant supporting tissues. The aim of this study is to review the latest periodontal perspectives on the treatment of peri-implantitis.
서론
2014년에 만 75세 이상을 대상으로 건강보험 임플란트를 시작한 이래로 만 65세 2개까지 지원을 확대하면서 의원급에서만 연간 60만 건에 달하는 건강보험 임플란트 시술이 이루어지고 있다. 2024년 12월을 기점으로 만 65세 이상 인구 비율이 20% 이상으로 초고령사회에 진입한 대한민국의 상황을 고려하면 고령인구에 대한 치과 임플란트 시술은 더 늘어날 것으로 생각된다.
임플란트 시술이 많아지면서 임플란트 주위염의 발생도 늘어나고 있다. 임플란트 주위염은 초기에는 치주염과 비슷한 질환 상태로 묘사되었지만, 관련 연구가 진행되면서 체계적으로 정의되고 있다[1]. 2017년에 열린 치주 및 임플란트 주변 질환 및 상태에 대한 세계 워크숍에서는 “치태로 인해 발생하는 병리학적 상태로, 임플란트 주위 점막의 염증이 나타나며, 점진적으로 임플란트 주변 골의 소실이 동반되는 질환”이라고 정의하였다[2]. 이러한 임플란트 주위염에 대해서 탐침 시 출혈, 탐침 깊이와 주변 치조골 상태에 따른 분류법을 대한치주과학회에서 2024년에 컨센서스 리포트로 출판하였다(Table 1) [3].
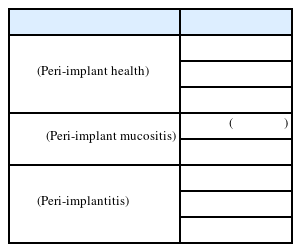
임플란트 주위염 분류 및 진단 기준
임플란트 주위염에 대한 치료 접근 방식은 일반적으로 치주염의 치료법과 유사하게 적용되고 있다[4]. 따라서 비수술적 및 외과적 치료를 통해 치태와 치석을 제거하고, 염증을 조절하며, 임플란트 주변 치주조직의 결합을 촉진하는 방향으로 시술한다.
이 연구의 목적은 고령화 사회에서 치과의사들이 놓치지 말아야 할 임플란트 주위염 치료의 최신 지견에 대한 치주과적 관점에서 살펴보고자 한다.
본론
비외과적 치료
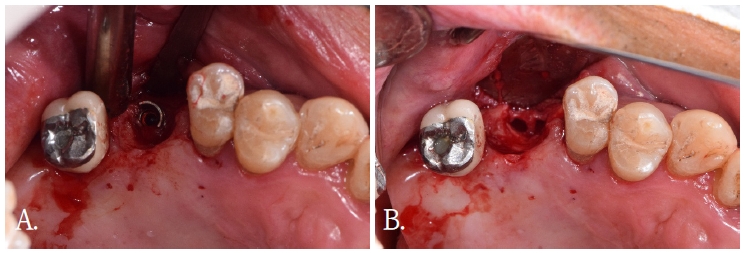
임플란트 주위 점막염은 임플란트 주위염의 전 단계로 여겨지며, 이는 치은염이 치주염의 전 단계로 판단하는 것과 비슷하다[5]. 비외과적 치료는 이러한 임플란트 주위 점막염의 관리에 효과적이며, 이는 임플란트 주위염으로의 진행을 예방하는 데 효과적이다[6]. 보편적으로 임플란트 주위 점막염의 치료에 기계적 괴사조직 제거술이 시술되었는데(Fig. 1), 질병의 진행 정도에 따라서 임플란트 주위염으로 진행되었을 때 시야 확보와 기구 접근이 제한되어 비외과적 치료만으로는 한계가 존재하여, 외과적 치료가 필요하게 된다[7].
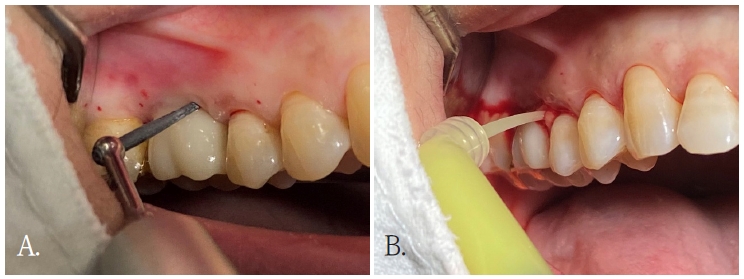
A. 임플란트 주위염 부위에 기계적 괴사조직 제거술을 진행하고 있다. B.기계적 괴사조직 제거술 진행 후 국소 전달 항생제를 부가 처치하고 있다.
그런데도 기계적 괴사조직 제거술에 보조적인 치료를 적용함으로써 비수술적 치료의 한계를 극복하려는 시도들이 있었다[8]. 레이저치료, 전신 항생제, 국소 전달 항생제(Fig. 1), 광생물 조절 요법, 광역학 요법 및 프로바이오틱스 같은 방법들이 기계적 괴사조직 제거술과 함께 시술되어 연구되었다[9].
레이저를 활용한 비외과적 치료에 대해 발표한 Alpaslan 등의 연구를 살펴보면, 기계적 괴사조직 제거술과 같이 Er,Cr:YSGG레이저를 시술했을 때, 탐침 시 출혈(BOP) 46% 감소(대조군 32%) 및 탐침 깊이(PD) 1.8mm 감소(대조군 1.2mm)세를 보였습니다. 또한 골 흡수 생체표지자(RANKL)의 유의미한 감소와 골 보호 효과(OPG/RANKL Ratio)가 증가함이 관찰되어 레이저 보조요법이 임플란트 주위염의 임상적, 생화학적 결과를 개선한다고 발표하였다[10].
치주질환 치료에서 항생제가 부가적인 치료로 사용되었을 때 성공적인 결과를 보여주어 임플란트 주위염의 치료에도 많은 연구가 진행되었다. 2022년에 발표된 국소 전달 항생제 및 전신 항생제의 부가적인 치료 효과에 대한 체계적 문헌 고찰 논문을 보면 국 전달 항생제는 치주낭 깊이와 임플란트 성공률에서 유의미한 개선이 나타났으나, 전신 항생제는 골 소실 감소는 보였지만 다른 수치에서는 유의미한 효과가 나타나지 않아 논란의 여지가 있다고 평가되었다[11]. 최근 연구에서 사용된 전신 항생제로는 메트로니다졸(500mg)이 방사선학적 뼈 증가와 염증 완화 그리고 치주 탐침 깊이 감소 등에서 유의미한 개선을 보였고, 국소 전달 항생제는 메트로니다졸과 미노사이클린을 함께 사용했을 때 임플란트 주위염 치료 성공률이 유의미하게 상승했다[4]. 하지만 보조적인 항생제의 과도한 사용은 항생제 내성을 향상할 위험이 있기 때문에 적절한 투여량과 사용기간의 고려가 필요하다.
외과적 치료
비외과적 치료 후에도 염증이 완전히 해소되지 않으면 외과적 치료를 시행하는데, 임플란트 주위염에 대한 외과적 치료는 접근 수술(access surgery), 절제 수술(resective surgery)과 재생 수술(regenerative surgery) 3가지로 분류된다[4].
1. 접근 수술
접근 수술은 치주 판막 거상을 통해 비외과적 치료의 한계를 직접 접근으로 극복하여 임플란트 표면의 오염을 제거한 후 치주 판막을 재위시키는 기본적인 외과적 치료 방식이다. 이 방법을 통해 오염된 임플란트 표면을 철저히 세정하여 세균 재정착을 최소화하고 재골융합(re-osseointegration)을 촉진을 도모한다[12].
기존에는 임플란트 표면 오염 제거에 금속 큐렛이나 초음파 스케일러가 사용되었으나, 티타늄 표면에 손상을 줄 수 있어 티타늄 큐렛, 플라스틱 팁이 장착된 초음파 스케일러, 에어 파우더 연마기, 회전식 티타늄 브러시 등이 제안되었다. 또한 표면 손상을 줄이려는 방법에 구연산, 과산화수소, EDTA, 클로르헥시딘 등의 화학적 세정제가 보조적으로 사용되는 연구들이 발표되고 있는데 어떤 화학제가 가장 효과적인가에 대해서는 논쟁이 있다[13].
2. 절제 수술
절제 수술은 임플란트 주위염에 이환된 골 결손부가 치조골에 잘 둘러싸여 있지 않거나 재생이 어려울 것으로 판단될 때 시행하는데, 술 후 환자의 구강 위생 관리를 용이하게 하려는 목적으로 시술된다.
절제 수술은 치주 판막 거상을 통해 접근성을 확보하고, 임플란트 주변 골 윤곽을 위생 관리에 용이하게 조정한다. 술 후에 노출될 것으로 예상되는 임플란트 나사선의 경우 나사선을 제거하고 표면을 매끄럽게 만드는 임플란트 성형술(implantoplasty)을 같이 시술하기도 한다(Fig. 2). 마지막으로 치주 판막의 위치를 재위치 시켜 치주낭 깊이 감소를 도모하는 과정으로 절제 수술은 진행된다[3].
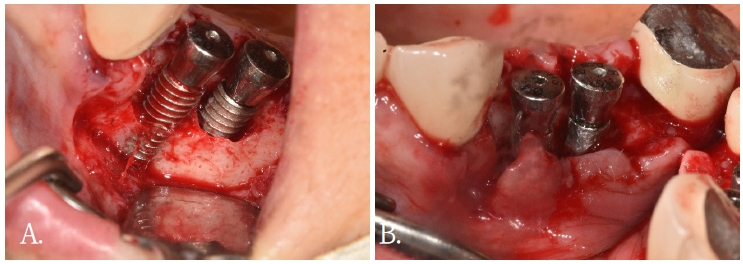
임플란트 주위염 부위에 임플란트 성형술을 시행하였다.
임플란트 성형술을 이용해 나사선을 제거하고 표면을 매끄럽게 만들면 노출되는 임플란트 표면에 미생물막 축적 및 박테리아 재성장을 크게 줄여 장기적인 안정성을 기대할 수 있다[14]. 반면에 표면을 연마하는 과정에서 발생하는 티타늄 입자가 완벽하게 제거되지 않아 생물학정 합병증을 일으키거나, 임플란트 구조를 얇게 만들어 파절의 위험성이 증가하는 단점이 보고되고 있다[3].
3. 재생 수술
재생 수술은 오염된 임플란트 표면을 세정한 후, 결손 부위를 골이식 재료로 충전하는 치료법이다(Fig. 3). Monje 등의 연구[15]에 따르면 결손부의 형태에 따라 예후가 크게 달라지며, 특히 원형 또는 2~3벽성 골 결손에서 재생 가능성이 높다고 발표했다. 또한 Froum 등[16]은 법랑질 유도 단백질이나 혈소판 유래 성장인자와 같은 성장인자와의 병용이 치료결과를 향상시킬 수 있다고 제안하였다.
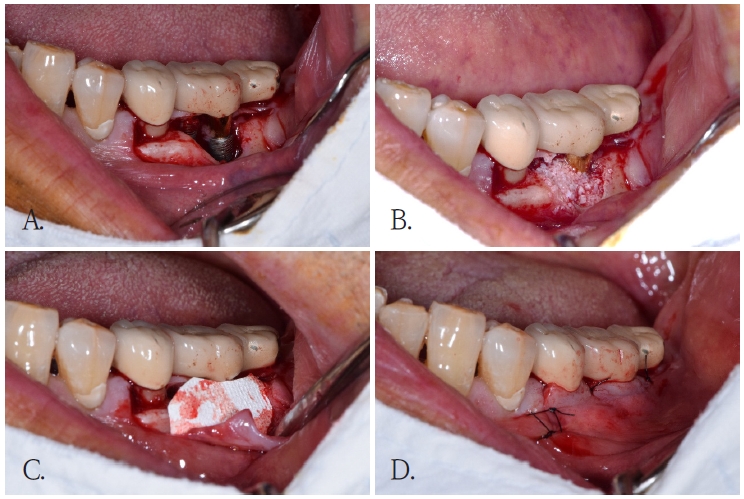
임플란트 주위염 부위에 골이식을 동반한 재생 수술을 시행하였다.
4. 연조직 이식의 병행
최근 임플란트 주위염 치료에 연조직 이식을 같이 시행한 증례들에 대한 체계적 문헌 고찰에 따르면 임플란트 주위염의 유병률을 낮춘다는 것이 조사되었다[17]. 이는 임플란트 주위 연조직의 질과 두께가 충분할 경우, 염증 재발을 줄이고 구강 관리에 도움이 되고, 연조직이 부족할 때 구강 청결 유지에 불편감을 느끼고 임플란트 주변 점막 밀폐(mucosal seal)를 저해한다는 기존의 연구가 반영된 것으로 판단된다.
따라서 임플란트 주위염에 외과적 치료를 진행할 때 필요시 연조직 이식(자가 조직 또는 콜라젠 대체물 사용) 을 병행하는 것이 권장된다.
결론
임플란트 주위염을 효과적으로 관리하기 위해서는 앞에서 살펴본 치료법도 중요하지만, 지속적인 재평가와 유지관리 치료가 매우 중요하다. 특히 고령 환자들의 경우 전신질환을 가지고 있거나, 구강 위생 관리에 어려움이 있어 각별한 관심이 필요하다.
고령 사회에서 임상가들은 임플란트 주위염에 대한 정확한 평가, 맞춤형 치료 계획 수립 및 체계적인 유지관리 프로토콜을 마련하여 질환의 재발을 예방하고 건강한 구강 위생 관리를 위한 교육을 병행하는 것이 추천된다.
Notes
Conflicts of Interest
None