IVRO의 술식은 다음과 같다. 절개는 하악 대구치 교합평면을 기준으로 상방 1cm 정도부터 전방으로 소구치 후방부까지 구강전정 상에 진행하고, 점막부터 골막까지를 포함하는 전층피판을 형성하여 상행지 측방의 피판을 거상한다. 상방으로는 S절흔(sigmoid notch), 하방으로는 우각부 하연, 후방으로는 상행지 후연까지 골점막을 완전히 벗겨 상행지의 측면을 완전히 노출시킨다. S절흔과 우각부 하연에 한쌍의 견인자(bauer’s retractor)를 걸어 상행지 측면에 oscillating saw가 들어갈 수 있는 공간을 확보한다. 노출된 상행지 측면에서 반소설돌기부(antilingular eminence)를 확인하고 후방으로 수직 골절단선의 방향과 위치를 표시한다().
Osteotomy design for intraoral vertical ramus osteotomy. The osteotomy line must be designed behind antilingular eminence.
이후 전동톱(oscillating saw)을 이용하여 반소설돌기부부터 하방으로 골절단을 시행하고 다시 위쪽으로 S절흔까지 약간의 전방 경사를 주어 골절단을 완성한다. 골편 사이의 완전한 분리를 확인하고 근심골편 내측에 부탁된 골막과 근육을 박리하고 근심골편이 원심골편의 외측에 중첩되도록 한다().
A. A pair of bauer retractors are placed at the sigmoid notch and the inferior border of the mandibular angle. B. Following vertical osteotomy, the mesial segment is overlapped laterally to the distal segment.
절단된 골편은 익돌근 교근 포(pterygomasseteric envelop)에 둘러싸인 해부학적 환경과 연가골이 형성되기 전까지 근심골편의 자유로운 움직임이 허용되는 독특한 환경 하에서 치유가 진행된다. 악간고정을 하지 않더라도 골편 사이의 치유에는 문제가 발생하지는 않지만, 술후 안정적인 교합을 완성하고 환자의 불편감을 줄이기 위해 통상 2주 정도의 악간고정(intermaxillary fixation)을 진행한다[10-13].
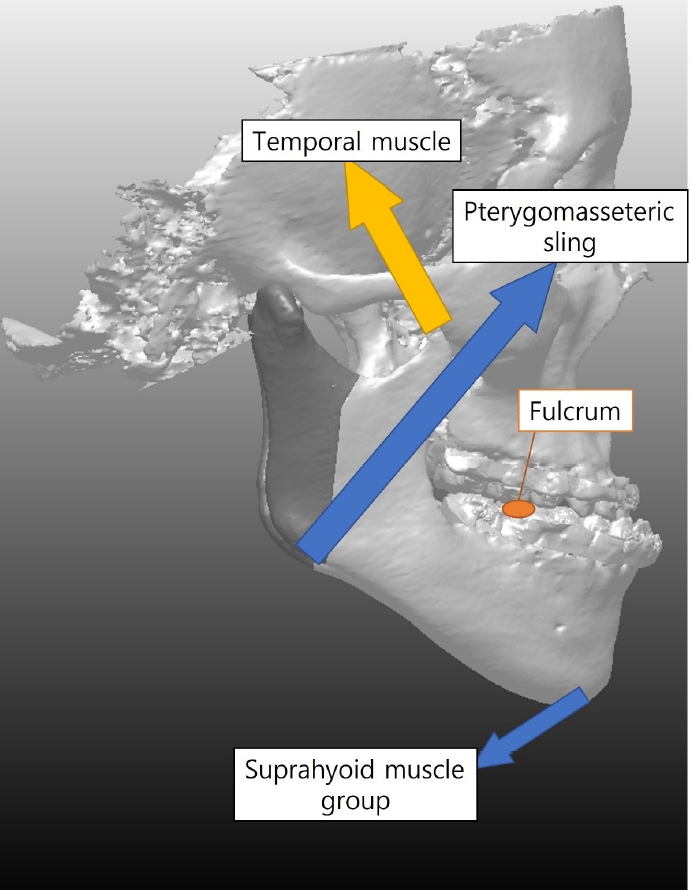
성공적인 IVRO 술식을 시행하기 위해서는 적절한 치료계획을 수립하여야 한다. 하악골의 근육돌기에는 측두근, 하악각에는 교근, 이부에는 suprahyoid muscle group이 부착된다. 이에 따라 IVRO 시행 후 측두근이 신전되는 방향(원심골편의 후방이 떨어져 상행지 길이가 늘어나는 방향)으로 수술 계획이 수립되는 경우 장기적으로 전방 개방교합이 반드시 발생하게 된다(). 이를 막기 위해서는 하악골 근육돌기가 후상방으로 위치되도록, 하악골 상행지가 길어지지 않는 방향으로 수술이 진행되도록 수술 계획을 반드시 수립하여야 한다().
Schematic diagram to understand the influence of mandibular muscles’ attachment on postoperative stability.
To ensure a stable occlusion following IVRO, the coronoid process should be moved posterio-superiorly as shown by the arrow.
IVRO의 특징 중 가장 두드러진 부분은 우선 하치조신경 손상 발생률이 매우 낮다는 점이다[14]. SSRO 시행 중 하치조신경의 완전 절단은 1.8-18 %에서 발생한다고 알려져 있고[15-18], SSRO와 관련된 신경손상으로 인한 감각이상 가능성은 85% 정도까지 보고된 바 있다[7,19,20]. 이에 비해 IVRO 후 신경 손상 가능성은 1% 미만으로 알려져 있다. IVRO에서 신경 손상 발생률이 낮은 이유는 골절단 부위를 하악공 후방에 유지함으로써 신경 손상을 쉽게 피할 수 있기 때문이다. 이에 추가로 IVRO를 진행할 때 보다 짧은 톱날을 사용하고, (CB)CT를 통한 길이와 두께를 확인함으로써 신경 손상 가능성을 더욱 낮출 수 있다.
계획된 골절선과 다르게 골절단이 시행된 경우를 예기치 않은 골절(bad split)이라 하며 시술이 복잡할수록 그 확률은 당연히 높아진다. 따라서 SSRO의 경우 bad split이 발생할 확률이 훨씬 높으며, 평균 약 2.3% 정도에서 발생한다고 알려져 있다[21,22]. 논란의 여지가 있지만 메타분석 결과 환자의 연령 증가가 예기치 않은 골절과 상관관계가 있는 것으로 알려져 있으며[22], 골편의 크기가 작거나 합병증이 발생할 경우 골수염 또는 부정유합의 발생가능성이 있음을 명심해야 한다.
IVRO 후 관절잡음, 통증 및 기타 턱관절 증상이 개선되는 것은 IMF 기간동안 턱관절과 주변 근육의 휴식, 관절강 내 압력저하때문일 가능성이 높으며, 이를 과두절제술 효과(condylotomy effect) 라 칭한다[23-28]. Jung 등[29] 은 IVRO 후 관절잡음이 70.8-94.3% 개선되었고, 턱관절 통증은 89.4%까지 개선되었다고 보고했다( and ). Ueki 등[30]의 MRI를 활용한 연구에서도 앞의 결과와 유사하게 SSRO에서는 개선된 효과가 없었지만 IVRO 후에는 50% 정도에서 관절원판 전방 변위가 정상으로 회복됨을 보고한 바 있다.
Chronological changes of temporomandibular joint (TMJ) sound following intraoral vertical ramus osteotomy [29]
Chronologic changes of temporomandibular joint (TMJ) pain following intraoral vertical ramus osteotomy [29]
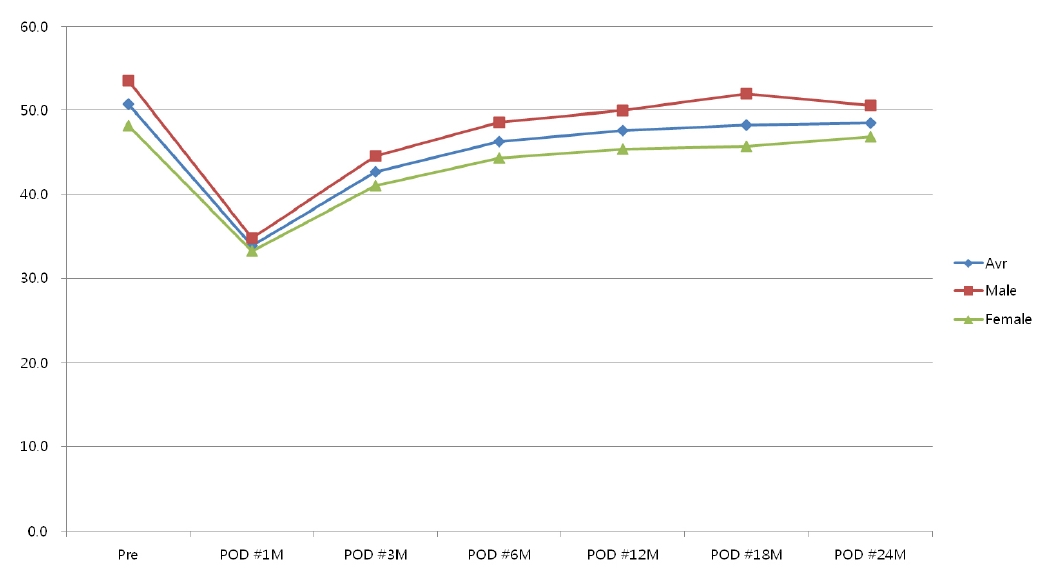
IVRO와 SSRO에서 모두 악간고정 기간이 짧을수록 수술 후 개구량 회복에 도움이 되는 것으로 알려져 있다[31]. 하지만, IVRO의 경우 연가골이 형성에 필요한 최소 시간이 7일이므로 환자의 편의와 안정적이고 신뢰할 수 있는 치유의 확보를 위해서는 2주 정도의 악간고정이 추천된다. 2주 정도의 악간 고정을 시행하더라도 적절한 물리치료를 진행한다면 개구량 회복에는 특별한 문제가 발생하지 않는다. Jung 등[32]은 IVRO 시행 후 수술 전 최대 개구량(maximum mouth opening)의 90%를 회복하는 데에는 약 6개월이 소요되었고, 통계적으로 수술 전 수준에 근접하는 데는 12개월이 소요된다고 보고하였다. 즉, IVRO 후 적절한 재활 물리치료를 적용하면 저작근의 재활과 하악 저운동성 개선에 도움이 된다고 생각할 수 있다.
수술 후 교정치료를 진행할 때 전후방적인 재발이 2.0mm를 초과하면 수술 후 치료기간이 늘어나고, 최종적으로 좋은 교합 상태를 완성하기 어렵다[33]. Costa 등[34] 은 3급 부정교합의 치료를 위해 SSRO를 이용한 경우 약 30.8%에서 2.0 mm 이상의 유의한 전방 재발(anterior relapse)이 있을 수 있다고 보고하였으며, profitt 등[35]은 2014년 발표된 논문에서 1995년 이후부터 지금까지 SSRO 수술적 기법의 계속적인 발전이 있었지만 아직까지 전방 재발과 관련해서는 결과가 만족스럽지 못하다고 보고한 바 있다. 이에 반해 IVRO의 경우 약간의 후방 재발(posterior relapse)이 발생함이 보고되고 있다[10,11,36]. Jung 등[37]의 연구에 따르면 IVRO 후 1년째에 menton은 상방으로 평균 3.0mm, 후방으로 평균 1.3mm 이동됨을 보고하였으며, 하악의 수술적 이동량과 재발량 사이의 상관관계가 없다고 보고하였다. 앞의 결과와 유사하게 SSRO와 IVRO를 이용한 randomized controlled trial을 진행한 Li 등[9] 도 수평적인 안정성은 SSRO보다 IVRO가 보다 우수하다고 보고하였다. 따라서, IVRO를 진행한다면 수술 계획 수립 시에 재발을 고려한 과교정(overcorrection)은 필요하지 않다. 그리고, IVRO 후에는 SSRO처럼 전방 재발이 잘 발생하지 않기 때문에 class III elastics 보다는 occlusal seating을 시키기 위한 수직 방향 또는 class II elastics를 적극적으로 활용하는 것이 바람직할 것이다.
IVRO의 가장 기본적인 단점은 악간 고정이 반드시 필요하다는 점이다. 하지만, 골편 사이의 가골이 형성되는 시기에 적절한 안정 기간만 확보된다면 치유 과정 상에 문제가 발생하는 경우는 없다[38]. 하루만 강선을 이용한 견고한 악간고정 후 고무줄 조기 적용을 해도 충분히 좋은 결과를 얻었다는 보고도 있지만[39], 골편 사이의 움직임을 느끼는 것 또한 환자에게 불편이 될 수 있기에 저자 등은 2주 정도의 악간고정 기간을 유지하는 것이 좋다고 생각한다.
IVRO 후 많은 사람들이 오해하는 내용 중 하악각 넓이 증가가 발생할 수 있다는 의문이다. 실재로 IVRO 후 근심골편은 외측으로 평균 15도 정도 회전하지만, 익돌근 교근 포에 둘러 쌓여있는 독특한 환경의 덕분으로 치유과정에서 점차 원래의 각도로 내회전되며 회복된다고 알려져 있다[40,41]. 그렇기 때문에 IVRO 후 하악각의 넓이는 경조직과 연조직 모두에서 넓어지지 않는다[42]. 하악각이 지나치게 발달해 있거나, 하악 후방 이동량이 과도하여 근심골편이 과도하게 외측으로 변위될 경우 수술 직후 하악각 넓이의 과도한 증가가 나타날 수도 있는데, 이런 경우는 J-VRO 또는 Y-VRO와 같은 변형된 형태로 수술 초기부터 심미적으로 개선된 상태를 만들어 낼 수 있을 것이다[43].
Chronologic changes of maximum mouth opening following intraoral vertical ramus osteotomy procedure[32].
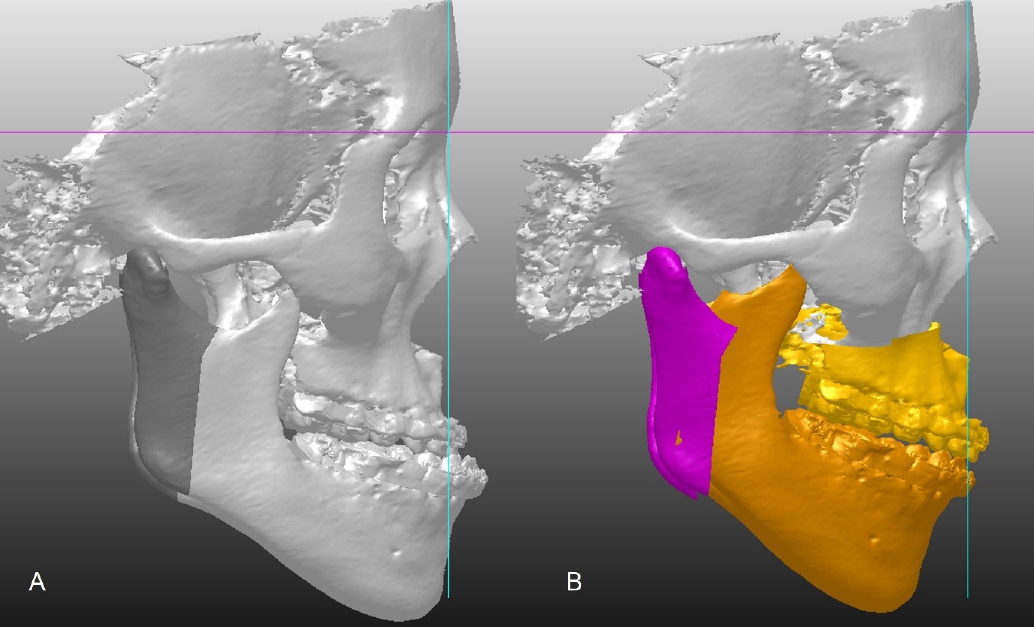
최근 심한 악안면 기형의 분석과 치료를 위해 3D simulation 및 CAD/CAM 기법이 널리 활용되고 있다[44-46]. 악교정수술 영역에서 SSRO와 IVRO 적용 시 수술 방법에 맞춰 골편의 골절선을 예측하고 수술 전 미리 시뮬레이션을 진행함으로써 수술 후 발생할 수 있는 합병증을 미리 예측하고 예방할 수 있다(). 3D simulation을 IVRO 수술 계획 시 활용하면, 하악공의 위치를 정확히 계측하여 하치조신경 손상을 미리 막을 수 있는 점, 안정성을 위해 근육돌기의 후상방 이동을 완벽히 만들어 낼 수 있는 점, 하악각 및 이부의 정확한 이동 위치를 미리 예상하여 심미적으로 보다 개선된 결과를 만들어 낼 수 있는 점 등을 장점으로 들 수 있다. 또한 과두의 형태나 안정성에 따라 수술 시 사용하는 장치의 형태를 변형하여 3D 프린팅이 가능하므로 보다 정확한 수술 결과를 만들어 내는 데 유리할 것이다[47]. 최근에는 전산유체역학(computational fluid dynamics), 기계학습, 인공지능 등을 활용하여 하악골 후퇴 후 기도공간 감소에 따른 수면무호흡증 발생에 대한 연구도 활발히 진행되고 있다[48-50].
Example of surgical planning using 3D simulation for intraoral vertical ramus osteotomy procedure.
IVRO는 하악골전돌증의 치료를 위해 하악의 원심 골편을 후방 이동할 때 이용할 수 있는 술식이다. 수직으로 절단된 근심 골편은 원심 골편의 외측으로 중첩되며 피질골-피질골 접촉을 하며 치유되는 과정을 거친다. IVRO는 SSRO에 비해[1] 술식이 간단하여 예기치 않은 골절이 발생할 가능성이 낮고[2], 수술시간이 짧으며[3], 하치조신경 손상 가능성이 낮고[4], 과두 절제술 효과를 통해 측두하악관절 질환의 개선에 유리하고[5,29,30], 전후방적 안정성이 상대적으로 유리하다[37]는 장점이 있다.
References
1. Alhammadi MS, Halboub E, Fayed MS, Labib A, El-Saaidi C. Global distribution of malocclusion traits: a systematic review. Dental Press J Orthod 2018;23:40.e1–10.
2. Trauner R, Obwegeser H. The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chin. Oral Surg Oral Med Oral Pathol 1957;10:677–89.
3. Hebert JM, Kent JN, Hinds EC. Correction of prognathism by an intraoral vertical subcondylar osteotomy. J Oral Surg 1970;28:651–3.
4. Wilbanks JL. Correction of mandibular prognathism by double-oblique intraoral osteotomy: a new technique. Oral Surg Oral Med Oral Pathol 1971;31:321–7.
5. Massey GB, Chase DC, Thomas PM, Kohn MW. Intraoral oblique osteotomy of the mandibular ramus. J Oral Surg 1974;32:755–9.
6. Hall HD, Chase DC, Payor LG. Evaluation and refinement of the intraoral vertical subcondylar osteotomy. J Oral Surg 1975;33:333–41.
7. MacIntosh RB. Experience with the sagittal osteotomy of the mandibular ramus: a 13-year review. J Maxillofac Surg 1981;9:151–65.
8. Teltzrow T, Kramer FJ, Schulze A, Baethge C, Brachvogel P. Perioperative complications following sagittal split osteotomy of the mandible. J Craniomaxillofac Surg 2005;33:307–13.
9. Li DT, Wang R, Wong NS, Leung YY. Postoperative stability of two common ramus osteotomy procedures for the correction of mandibular prognathism: a randomized controlled trial. J Craniomaxillofac Surg 2022;50:32–9.
10. Greebe RB, Tuinzing DB. Overcorrection and relapse after the intraoral vertical ramus osteotomy. A one-year postoperative review of thirty-five patients. Oral Surg Oral Med Oral Pathol 1982;54:382–4.
11. Ayoub AF, Millett DT, Hasan S. Evaluation of skeletal stability following surgical correction of mandibular prognathism. Br J Oral Maxillofac Surg 2000;38:305–11.
12. Lai SS, Tseng YC, Huang IY, Yang YH, Shen YS, Chen CM. Skeletal changes after modified intraoral vertical ramus osteotomy for correction of mandibular prognathism. J Plast Reconstr Aesthet Surg 2007;60:139–45.
13. Chen CM, Lee HE, Yang CF, Shen YS, Huang IY, Tseng YC, et al. Intraoral vertical ramus osteotomy for correction of mandibular prognathism: long-term stability. Ann Plast Surg 2008;61:52–5.
14. Al-Bishri A, Barghash Z, Rosenquist J, Sunzel B. Neurosensory disturbance after sagittal split and intraoral vertical ramus osteotomy: as reported in questionnaires and patients' records. Int J Oral Maxillofac Surg 2005;34:247–51.
15. Turvey TA. Intraoperative complications of sagittal osteotomy of the mandibular ramus: incidence and management. J Oral Maxillofac Surg 1985;43:504–9.
16. van Merkesteyn JP, Groot RH, van Leeuwaarden R, Kroon FH. Intra-operative complications in sagittal and vertical ramus osteotomies. Int J Oral Maxillofac Surg 1987;16:665–70.
17. Agbaje JO, Salem AS, Lambrichts I, Jacobs R, Politis C. Systematic review of the incidence of inferior alveolar nerve injury in bilateral sagittal split osteotomy and the assessment of neurosensory disturbances. Int J Oral Maxillofac Surg 2015;44:447–51.
18. Westermark A, Bystedt H, von Konow L. Inferior alveolar nerve function after mandibular osteotomies. Br J Oral Maxillofac Surg 1998;36:425–8.
19. Nishioka GJ, Zysset MK, Van Sickels JE. Neurosensory disturbance with rigid fixation of the bilateral sagittal split osteotomy. J Oral Maxillofac Surg 1987;45:20–6.
20. Walter JM, Gregg JM. Analysis of postsurgical neurologic alteration in the trigeminal nerve. J Oral Surg 1979;37:410–4.
21. Steenen SA, Becking AG. Bad splits in bilateral sagittal split osteotomy: systematic review of fracture patterns. Int J Oral Maxillofac Surg 2016;45:887–97.
22. Steenen SA, van Wijk AJ, Becking AG. Bad splits in bilateral sagittal split osteotomy: systematic review and meta-analysis of reported risk factors. Int J Oral Maxillofac Surg 2016;45:971–9.
23. Boyd SB, Karas ND, Sinn DP. Recovery of mandibular mobility following orthognathic surgery. J Oral Maxillofac Surg 1991;49:924–31.
24. Hall HD, McKenna SJ. Further refinement and evaluation of intraoral vertical ramus osteotomy. J Oral Maxillofac Surg 1987;45:684–8.
25. Ueki K, Marukawa K, Shimada M, Hashiba Y, Shimizu C, Nakgawa K, et al. Condylar and disc positions after intraoral vertical ramus osteotomy with and without a Le Fort I osteotomy. Int J Oral Maxillofac Surg 2007;36:207–13.
26. Bell WH, Yamaguchi Y. Condyle position and mobility before and after intraoral vertical ramus osteotomies and neuromuscular rehabilitation. Int J Adult Orthodon Orthognath Surg 1991;6:97–104.
27. Astrand P, Ericson S. Relation between fragments after oblique sliding osteotomy of the mandibular rami and its influence on postoperative conditions. Int J Oral Surg 1974;3:49–59.
28. Egyedi P, Houwing M, Juten E. The oblique subcondylar osteotomy: report of results of 100 cases. J Oral Surg 1981;39:871–3.
29. Jung HD, Jung YS, Park HS. The chronologic prevalence of temporomandibular joint disorders associated with bilateral intraoral vertical ramus osteotomy. J Oral Maxillofac Surg 2009;67:797–803.
30. Ueki K, Marukawa K, Nakagawa K, Yamamoto E. Condylar and temporomandibular joint disc positions after mandibular osteotomy for prognathism. J Oral Maxillofac Surg 2002;60:1424–32.
31. Ueki K, Marukawa K, Hashiba Y, Nakagawa K, Degerliyurt K, Yamamoto E. Assessment of the relationship between the recovery of maximum mandibular opening and the maxillomandibular fixation period after orthognathic surgery. J Oral Maxillofac Surg 2008;66:486–91.
32. Jung HD, Jung YS, Park JH, Park HS. Recovery pattern of mandibular movement by active physical therapy after bilateral transoral vertical ramus osteotomy. J Oral Maxillofac Surg 2012;70:e431–7.
33. Proffit WR, Phillips C, Dann Ct, Turvey TA. Stability after surgical-orthodontic correction of skeletal class III malocclusion. i. mandibular setback. Int J Adult Orthodon Orthognath Surg 1991;6:7–18.
34. Costa F, Robiony M, Politi M. Stability of sagittal split ramus osteotomy used to correct class III malocclusion: review of the literature. Int J Adult Orthodon Orthognath Surg 2001;16:121–9.
35. Proffit WR, Phillips C, Turvey TA. Stability after mandibular setback: mandible-only versus 2-jaw surgery. J Oral Maxillofac Surg 2012;70:e408–14.
36. Yoshioka I, Khanal A, Tominaga K, Horie A, Furuta N, Fukuda J. Vertical ramus versus sagittal split osteotomies: comparison of stability after mandibular setback. J Oral Maxillofac Surg 2008;66:1138–44.
37. Jung HD, Jung YS, Kim SY, Kim DW, Park HS. Postoperative stability following bilateral intraoral vertical ramus osteotomy based on amount of setback. Br J Oral Maxillofac Surg 2013;51:822–6.
38. Jung HD, Kim SY, Jung HS, Park HS, Jung YS. Immunohistochemical analysis on cortex-to-cortex healing after mandibular vertical ramus osteotomy: a preliminary study. J Oral Maxillofac Surg 2018;76:437e1–8.
39. Ohba S, Tasaki H, Tobita T, Minamizato T, Kawasaki T, Motooka N, et al. Assessment of skeletal stability of intraoral vertical ramus osteotomy with one-day maxillary-mandibular fixation followed by early jaw exercise. J Craniomaxillofac Surg 2013;41:586–92.
40. Choi YS, Jung HD, Kim SY, Park HS, Jung YS. Remodelling pattern of the ramus on submentovertex cephalographs after intraoral vertical ramus osteotomy. Br J Oral Maxillofac Surg 2013;51::e259–62.
41. Song SH, Kim JY, Lee SH, Park JH, Jung HD, Jung YS. Three-dimensional analysis of transverse width of hard tissue and soft tissue after mandibular setback surgery using intraoral vertical ramus osteotomy: a retrospective study. J Oral Maxillofac Surg 2019;77:407.e1–6.
42. Jung YS, Kim SY, Park SY, Choi YD, Park HS. Changes of transverse mandibular width after intraoral vertical ramus osteotomy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:25–31.
43. Jung HD, Kim SY, Park HS, Jung YS. Modification of intraoral vertical ramus osteotomy. Br J Oral Maxillofac Surg 2014;52:866–7.
44. Marchetti C, Bianchi A, Bassi M, Gori R, Lamberti C, Sarti A. Mathematical modeling and numerical simulation in maxillo-facial virtual surgery (VISU). J Craniofac Surg 2006;17:661–8.
45. Swennen GR, Mommaerts MY, Abeloos J, De Clercq C, Lamoral P, Neyt N, et al. A cone-beam CT based technique to augment the 3D virtual skull model with a detailed dental surface. Int J Oral Maxillofac Surg 2009;38:48–57.
46. Dai J, Tang M, Xin P, Hu G, Si J, Dong Y, et al. Accurate movement of jaw segment in virtual 3D orthognathic surgery. Int J Oral Maxillofac Surg 2014;25:e140–3.
47. Park JH, Lee YB, Kim SY, Kim HJ, Jung YS, Jung HD. Accuracy of modified CAD/CAM generated wafer for orthognathic surgery. PLoS One 2019;14e0216945.
48. Park JH, Kim HS, Choi SH, Jung YS, Jung HD. Changes in position of the hyoid bone and volume of the pharyngeal airway after mandibular setback: three-dimensional analysis. Br J Oral Maxillofac Surg 2019;57:29–35.
49. Ryu S, Kim JH, Yu H, Jung HD, Chang SW, Park JJ, et al. Diagnosis of obstructive sleep apnea with prediction of flow characteristics according to airway morphology automatically extracted from medical images: computational fluid dynamics and artificial intelligence approach. Comput Methods Programs Biomed 2021;208:106243.
50. Yeom SH, Na JS, Jung HD, Cho HJ, Choi YJ, Lee JS. Computational analysis of airflow dynamics for predicting collapsible sites in the upper airways: machine learning approach. J Appl Physiol 2019;127:959–73.