상악동에 발생한 콜레스테롤 육아종 증례 보고
Case report of cholesterol granuloma in the maxillary sinus
Article information

Trans Abstract
Cholesterol granuloma is known to be a disease formed by hemosiderin and cholesterol crystals when bleeding occurs while ventilation and drainage are not well performed by inflammatory tissue. It is known to occur mainly inside the temporal bone that has been undergone pneumatization, and occurrences in the paranasal sinuses have been rarely reported. A 72-year-old female patient visited to our institution, complaining of a sensation that pus had been coming out of her upper right extraction sockets for the past few months ago. She underwent the extraction of her upper right first and second molars a year ago. In the CBCT image, a well-circumscribed and expansile cystic lesion was located in the right maxillary sinus, bulging posterolateral wall of the maxillary sinus, with amorphous internal calcification and sclerotic border. After surgical excision, the lesion was confirmed as cholesterol granuloma with massive ossification by the histopathological interpretation postoperatively.
Ⅰ. 서론
콜레스테롤 육아종(cholesterol granuloma)은 1894년 Manasse [1]에 의해 처음으로 보고되었으며 중이강(middle ear cavity), 유돌봉소(mastoid air cell) 및 부비동(paranasal sinus) 등의 함기화가 진행된 공간에서 발생할 수 있으며 염증조직에 의해 환기와 배액이 잘 이루어지지 않는 상태에서 출혈이 발생하는 경우, 적혈구가 분해되어 축적되는 혈철소(hemosiderin)와 콜레스테롤 결정체에 의한 육아종성 반응으로 형성되는 질환으로 알려져 있다[2]. 콜레스테롤 육아종은 함기화가 진행되어 있는 모든 신체 부위에서 발생할 수 있고 특히 측두골의 내부에서 자주 발생하는 것으로 알려져 있는 반면에, 상악동을 비롯한 부비동에서의 발생은 매우 드물게 보고된 바 있다[3]. 특히 국내 치의학 관련 문헌에서 하악골에서 발생한 콜레스테롤 육아종에 대한 2개의 증례 보고가 확인되었으나[4,5], 상악동에서 발생한 콜레스테롤 육아종에 대한 증례는 보고된 바가 없는 것으로 확인되었다.
저자들은 상악동에서 수술적 처치 후 병리조직학적 소견 상 콜레스테롤 육아종으로 진단된 증례를 보고하고, 동시에 문헌고찰을 통해 해당 병소에서 관찰되는 특징을 소개하고자 한다.
Ⅱ. 증례
이 증례보고는 조선대학교치과병원 기관생명윤리위원회에서 승인 번호 CUDHIRB 2401 003으로 승인을 받았다. 72세의 여자 환자가 1년 전 우측 상악 제1,2 대구치 발거 후, 수개월 동안 지속해서 해당 부위에서 염증 삼출물이 나온다는 증상을 호소로 조선대학교 치과병원에 내원하였다. 처음 내원했을 때, 양측 상악 제1, 2대구치(#16,17,26,27)는 결손된 상태였고 임상 검사에서 발치 후 치유가 완전하게 진행된 정상 구강 점막의 형태를 관찰할 수 있었다. 환자는 전신 질환으로 고혈압과 당뇨가 있었으며, 안면부 외상이나 상악동 수술 등의 병력은 존재하지 않았다.
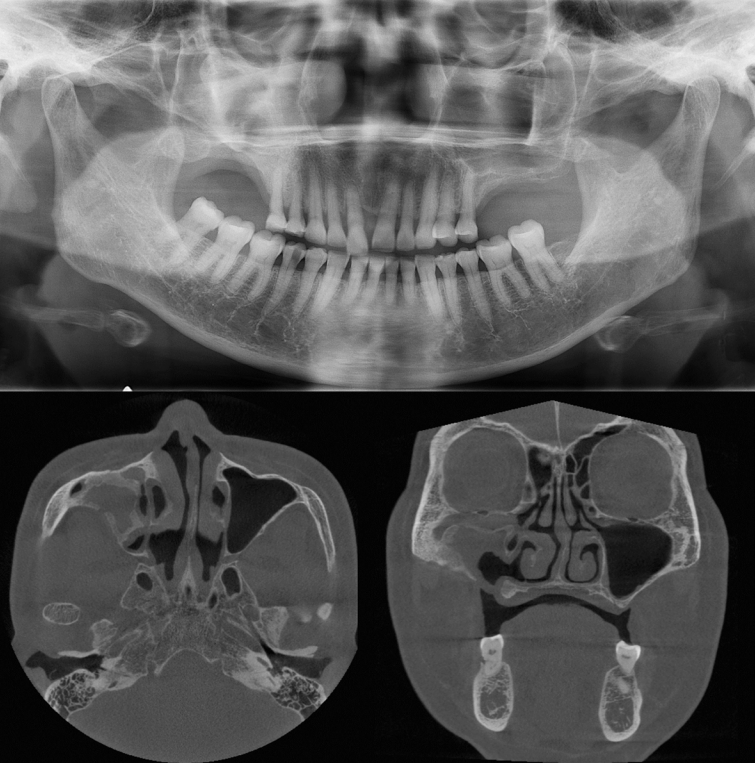
파노라마방사선영상에서 우측 상악동 내부 대부분의 공간이 방사선불투과상으로 채워져 있는 것을 관찰할 수 있었다(Fig. 1). 또한 반대측과 비교하였을 때 우측 상악동 저의 경계가 분명하지 않고 치조골의 골밀도가 감소된 소견을 보였다. 추가적인 평가를 위해 cone-beam computed tomography(CBCT)에서 얻어진 영상을 axial, coronal, panoramic plane으로 재구성하였다. 재구성된 영상에서 우측 상악동 내부를 채우고 있는 장경 3.5 cm정도의 낭종 병소가 관찰되었으며, 상악동의 전방 및 후외측 골이 팽융되고 상악동의 후외측 경계와 상악 치조골이 병소에 의해 소실된 소견이었다(Fig. 2). 병소의 경계는 대체적으로 잘 구분되고 타원 형태의 구조를 보였다. 경계 부위에서는 비후된 형태의 경화성 골 변연이 관찰되었고 병소 내부에서는 불규칙하고 무정형의 석회화가 산재되어 있었다. 술후상악낭(postoperative maxillary cyst)과 석회화치성낭(calcifying odontogenic cyst)을 감별진단으로 고려하였다.
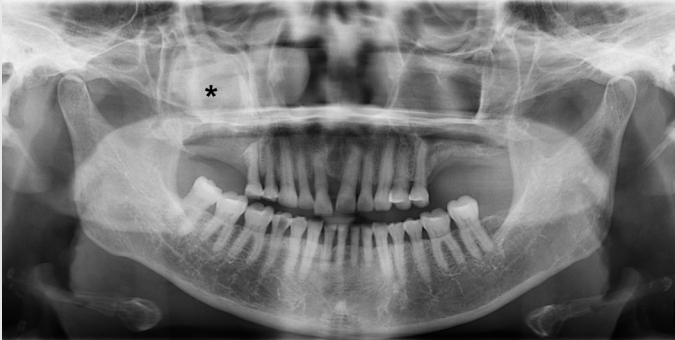
There is a haziness in the right maxillary sinus (*) with bony bulging at the posterior margin of the sinus and the bone density of the upper right alveolar bone is also reduced.
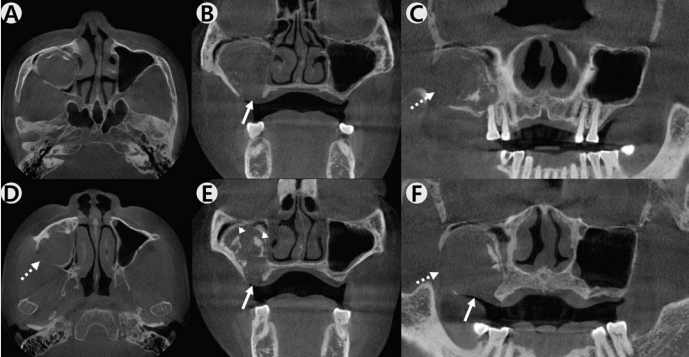
Expansile, soft tissue density mass is located in the right maxillary sinus from the reconstructed CBCT axial (A,D), coronal (B,E), panoramic (C,F) planes. There is an amorphous calcification within the mass (arrow head). Loss of the floor of the maxillary sinus (arrow) is observed and posterolateral wall of the maxillary sinus is also absent (dashed arrow).
본원 구강악안면외과에서 전신마취 하 구강 내 치조정측 접근을 통한 수술적 적출을 시행하였는데, 수술하면서 우측 상악동에서 농이 배출되는 양상과 육안상으로 볼 때 육아종처럼 보여지는 종괴(granulative mass)를 관찰할 수 있었다(Fig. 3). 수술 후 병리조직학적 검사 결과, 광범위한 골화를 동반한 콜레스테롤 육아종(cholesterol granuloma with massive ossification)으로 진단되었다(Fig. 4).
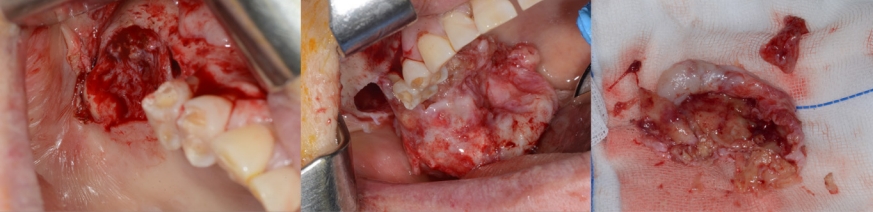
A granulative mass is observed at the operation site.
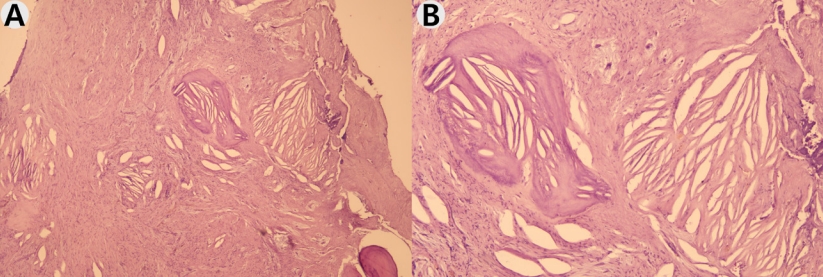
Hematoxylin and eosin (H&E) staining is performed and cholesterol clefts with ossification is observed at 40x (A), 100x (B) magnification.
환자는 수술 후 약 2주 정도 수술 부위에 대한 관리와 상악동의 배농 및 환기 상태의 유지를 위해 추가적인 처치를 받은 후 퇴원하였고, 수술 8개월 후 시행한 CBCT 검사에서 재발과 관련된 소견이 관찰되지 않았으며(Fig. 5) 현재까지 별다른 합병증 없이 추적 관찰 중이다.
There are no specific complications after 8 months following the operation.
Ⅲ. 고찰
콜레스테롤 육아종은, 환기장애 및 배설장애로 인해 폐쇄되어 있는 공간의 내부에서 음압이 발생하고 이로 인한 점막 부종과 미세한 출혈이 콜레스테롤 열(cleft)을 생성하게 된다고 알려져 있다[8]. 혈관의 분포가 풍부한 부비동이나 비중격 점막하에서는 혈액 유출의 가능성이 높으며, 점막 부종 및 용종으로 인해 부비강의 폐쇄로 이어질 수 있고, 음압으로 인한 혈관 외 유출이 발생하면 콜레스테롤 육아종이 생길 수 있다[9]. 본 증례의 경우 환자의 우측 상악 대구치의 발치와 관련하여 우측 상악동에서 점막 비후를 동반한 염증 반응이 발생했을 가능성을 고려해볼 수 있다. 병소의 치료와 관련되어 배액과 환기 체계의 확립을 원칙으로 하는데, 재발의 방지를 위해 완전한 절제술과 조대술 중 어느 것이 좋은 방법인가에 관해서는 논란이 있으나 병소의 위치에 따라 완전 절제가 어려운 경우가 많으며 주위로 확장하는 경우가 드물고, 상피세포 없이 섬유성 조직으로 낭벽이 이루어져 있어 재발이 드물기에 낭벽을 완전 절제할 필요 없이 조대술로 충분하다고 알려져 있다[12].
부비동에서 발생하는 콜레스테롤 육아종은 거대세포, 염증세포, 혈철소, 콜레스테롤을 함유한 대식세포 등이 특징적인 병리조직학적 소견에 의해 진단이 가능하며 임상 증상이나 영상학적 소견만으로는 진단이 어려울 수 있다. 본 증례의 영상 소견에서는, 병소가 상악동 내부에 위치하며 경계가 비교적 분명하고 타원 형태를 보이며, 내부에서는 무정형의 석회화를 보이는 소견이 관찰되었다. 이러한 병소의 형태적인 특징으로 미루어 술후상악낭 혹은 석회화치성낭을 고려하였으나 수술 후 병리조직학적 소견 상 광범위한 골화를 동반한 콜레스테롤 육아종으로 최종 진단되었다. 특히 기존의 다른 문헌들과 달리, 본 증례에서만 관찰되었던 특징적인 소견인 병소 내부의 석회화 소견은, 조직검사결과에서 광범위한 골화(massive ossification)로 진단되었다. 현재까지 국내에 보고된 문헌 중에서 본 증례의 병소와 같이 상악동의 콜레스테롤 육아종에서 골화(ossification)을 보이는 소견은 존재하지 않았다. 정확한 기전에 대해 확신하기는 어렵지만 저자들이 추측하기로는, 지속된 염증 상태에 의해 골 화생(osseous metaplasia)이 발생했을 것으로 보인다.
자기공명영상에서 콜레스테롤 육아종의 혈철소(hemosiderin)와 콜레스테롤 성분으로 인하여 T1 및 T2 강조영상 모두에서 고강도 신호를 보인다고 알려져 있는데[7,10,11] 본 증례에서는 자기공명영상 검사를 시행하지 않아 CBCT 영상 소견에 의존할 수밖에 없었다. 이 질환의 감별 진단을 위해 자기공명영상 검사를 시행한다면 병소 내부 성상에 대한 정보를 얻을 수 있어 감별 진단에 도움이 되는 것은 물론, 보다 정확한 진단과 치료를 기대해 볼 수 있을 것 같다.