임플란트-고정체 지지 형태의 티타늄-메쉬를 이용한 수직적 치조골 증식술 : 증례 보고
Vertical Alveolar Ridge Augmentation using fixture-supported Titanium-mesh : Case Series
Article information

Trans Abstract
The vertical height of the alveolar bone and the amount of remaining bone are important factors in the long-term success of implants. If the remaining bone is insufficient, procedures such as vertical alveolar ridge augmentation, like guided bone regeneration, are necessary for ideal implant surgery. Among the non-resorbable membranes that can be used in these procedures, titanium mesh offers advantages such as maintaining space for bone grafting, protecting the underlying graft material, and allowing adjustment to match the defect site for desired shaping. However, fixation of titanium mesh, which is crucial in determining the overall success of the surgery, requires the use of multiple screws and may result in membrane exposure during the healing process. To overcome these problems, a recent development involves the use of fixture-supported titanium-mesh, which has demonstrated good results. This study suggests that vertical alveolar ridge augmentation using fixture-supported titanium mesh can resolve conventional problems and can be considered an effective and reasonable strategy for achieving ideal implants.
Ⅰ. 서론
현재 치아 상실 부위를 임플란트로 대체하는 것은 일반적이고 예지성 있는 치료법이다. 임플란트 식립을 위한 잔존골 양은 임플란트의 장기적인 성공과 심미적 측면뿐만 아니라 추후 보철에서도 중요한 역할을 한다. 수평적으로는 최소 4mm, 수직적으로는 최소 7mm의 잔존골이 필수적이며, 잔존골의 양이 충분하지 않으면 기능적이고 심미적인 문제가 발생할 수 있다[1].
이러한 문제를 해결하기 위해 다양한 수술적 접근법이 개발되었다. 이 중에서도 골 유도 재생술(GBR)은 흡수성 및 비흡수성 차폐막을 활용하여 연조직이 골 결손부로 성장하는 것을 방지하고, 골 형성 세포 집단만이 결손부의 공간을 채울 수 있도록 한다[2]. 골 유도 재생술의 여러 장점에도 불구하고, 적절한 차폐막을 이용하여 골 증식을 위한 공간을 유지하는 것은 어려운 일이다. 이러한 상황에서 효과적으로 사용될 수 있는 티타늄-메쉬는 비흡수성 차폐막 중 하나로, 1969년 Boyne에 의해 처음 도입되어 치조골의 수평 및 수직적 증식에 사용하였다[3].
티타늄-메쉬 차폐막은 높은 강성, 낮은 밀도, 부식 저항성 및 우수한 생체 적합성 등의 특성을 가지며, 조작성이 좋아서 골 결손 부위에 맞게 조정하고 원하는 형태를 형성할 수 있다. 또한, 골 이식한 공간을 유지하는데 유리하며, 막 하부에 있는 이식편을 보호하여 치유기간 동안 연조직의 붕괴와 이식편의 압박 또는 변위를 방지할 수 있다[4,5]. 게다가, 티타늄-메쉬는 노출 비율이 낮고 노출 시에도 구멍이 존재하여 혈류를 방해하지 않아 즉시 제거가 필요하지 않다[6].
티타늄-메쉬를 이용한 치조골 증식술에서 중요한 것은 차폐막의 고정이다. 고정이 잘 되지 않는다면, 연조직의 개입으로 골형성을 방해하며, 감염 또한 발생할 수 있다. 이에 따라, 티타늄-메쉬의 고정을 위한 다양한 방법들이 보고되었지만 술식의 난이도가 다양하고, 임플란트 고정체 식립을 동시에 하지 못하는 경우도 있다. 이러한 문제를 해결하기 위해 최근 티타늄-메쉬를 직접 임플란트 고정체에 고정하는 형태의 골 증식술이 관심을 받고 있다.
본 증례보고에서는 임플란트 고정체 지지 형태의 티타늄-메쉬를 이용하여 임플란트 고정체 식립과 동시에 수직적 치조골 증식술을 시행하여 만족할 만한 결과를 보인 증례를 보고하여 도움이 되고자 한다. 특히, 일차적인 치조골 이식술을 실패한 증례에서 임플란트 식립과 동시에 고정체 지지 형태의 티타늄-메쉬를 이용한 치조골 증식술에 유용한 결과를 얻어 함께 보고하고자 한다.
Ⅱ. 증례보고
Case 1
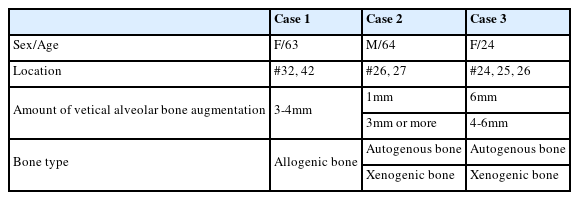
만 63 세의 여성 환자가 교통사고로 인한 하악 4전치의 탈구 및 하악 전치부의 치조골 골절로 내원하였다. 턱 및 좌측 협점막의 열상이 동반되어 있었으며, 과거력으로 고지혈증을 제외하고 특이 병력은 없었다. 열상에 대한 일차 봉합술 및 치조골 골절 부위의 파편을 제거하였으며, #31, 32, 41, 42의 잔존 치근 발치를 시행하였다. 잔존 치근 발치 후 3개월의 치유기간을 두고 치과용 panorama 방사선 사진 및 콘빔 CT(Cone-beam computed tomography)를 촬영하였고, 치조골의 낮은 수직적인 높이로 인해 수직적 치조골 증식술과 함께 하악 좌측 측절치(#32), 하악 우측 측절치(#42) 부위의 임플란트 1차 수술을 계획하였다(Fig. 1A, B, C).
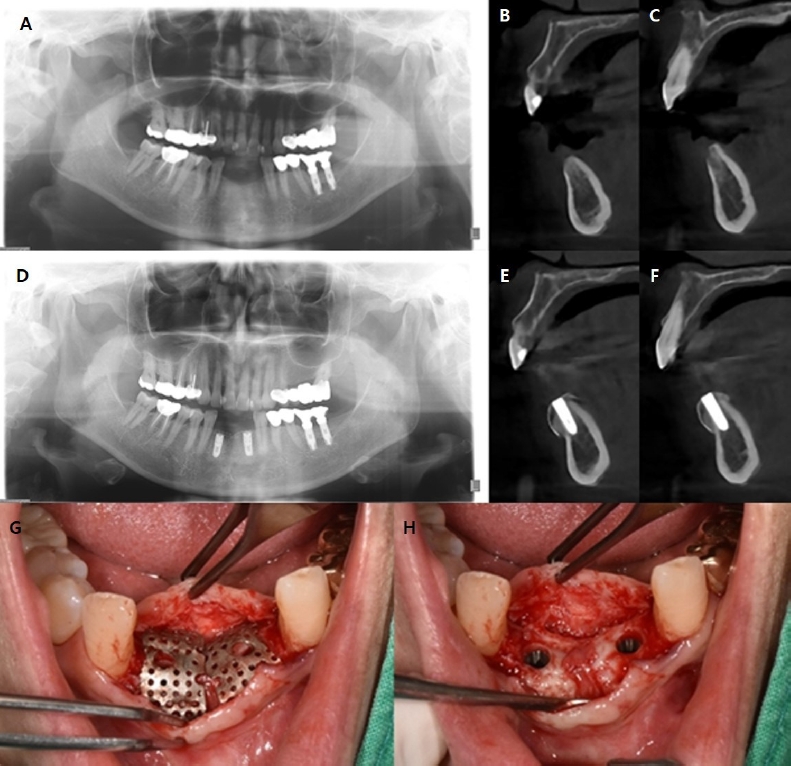
(A) Panoramic radiography of the patient taken before the surgery, It shows vertical alveolar bone loss on mandibular anterior area. Cone beam computed tomography (B,C) of the patient taken before the surgery (B) Sagittal view of #32 area. (C) Sagittal view of #42 area. (D) Panoramic radiography of the patient taken after four month of the surgery, It shows an increase in the level of alveolar bone. Cone beam computed tomography (E,F) of the patient taken after four month of the surgery (E) Sagittal view of #32 area , (F) Sagittal view of #42 area shows 3mm of vertical alveolar bone augmentation & 3-4mm of horizontal alveolar bone augmentation. (G) Clinical photo before titanium mesh removal. (H) Clinical photo after titanium mesh removal, vertical and horizontal alveolar bone augmentation is observed.
치은의 절개 및 판막 거상 후 하악 좌측 측절치(#32) 부위(TSIII Mini 3.5 x 10.0mm, Osstem, Seoul, South Korea) 및 하악 우측 측절치(#42) 부위(TSIII Mini 3.5 x 10.0mm, Osstem, Seoul, South Korea)의 임플란트 고정체를 식립하였다. 그 후, 임플란트-고정체 지지 형태의 티타늄-메쉬(OssBuilder, OB3 10[P] x 9[BW] x 9[BL], OB3 10[P] x 9[BW] x 4.5[BL], Osstem, Seoul, South Korea)를 골 이식 후 원하는 형태에 맞게 조정하여 윤곽을 잡았다. 골 이식에는 동종골 이식재(DO Bone™ 0.5cc * 2개 , DO Bone™, Renewmedical, Seoul, South korea) 가 사용되었다. 골 이식물은 티타늄-메쉬 하부에 위치하였으며, 티타늄-메쉬는 식립된 임플란트 고정체의 지지를 받아, 골 이식재를 고정하였다. 그 후 거상하였던 판막을 봉합하였다. 수술 후 관리에는 항생제(1세대 세팔로스포린계) 및 진통제 사용이 포함되었으며, 수술 7일 후에 발사하였다.
치유 단계 중 감염 등의 임상적 증상은 없었으며, 4개월의 치유기간 동안 티타늄-메쉬의 노출은 관찰되지 않았다. 시행한 방사선 검사상, 골이식을 시행한 하악 좌측 측절치(#32) 부위 및 하악 우측 측절치(#42) 부위의 3mm의 수직적 골증식 및 3~4mm 정도의 수평적 골증식을 확인하였다(Fig. 1D, E, F). 치유기간 동안 골증식이 일어난 부위의, 비흡수성 차폐막인 티타늄-메쉬는 제거되었으며, 수직 및 수평적 골증식을 확인하였다(Fig. 1G, H). 동시에 하악 좌측 측절치(#32) 및 하악 우측 측절치(#42) 부위의 임플란트에 Healing abutment(4.0 x 7mm mini, Osstem, Seoul, South Korea) 체결을 통한 2차수술을 시행하였으며, 7일 후 발사하였다.
Case 2
만 64세의 남성 환자가 좌측 상악 구치부의 임플란트 식립을 주소로 내원하였다. 과거력으로 약 8년전 postoperative maxillary cyst(POMC)에 대한 낭종 적출술 및 #26, 27 발치를 시행하였었다. 임상 검사 및 방사선 검사상 주소부위의 Scar tissue 및 상당한 수평 및 수직적 치조골 소실이 관찰되어, 우선적으로 좌측 상악 구치부의 Scar tissue 제거 및 하악지의 자가골 이식술을 계획하였다(Fig. 2A, B).
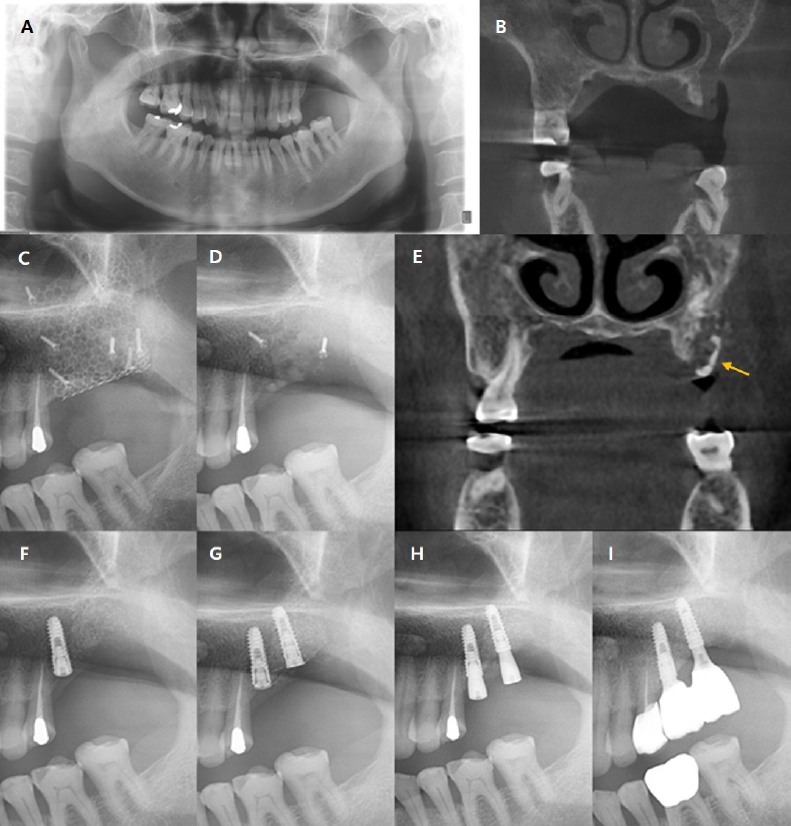
(A) Panoramic radiography of the patient taken before the surgery, It shows vertical alveolar bone defect on Lt. Mn. post. area. (B) Cone beam computed tomography of the patient taken before the surgery. (C) After ramal bone graft surgery with titanium mesh. (D,E) Infected ramal bone (arrow), loosening of micro screws and titanium mesh was observed. After removing all of them, unsatisfactory alveolar bone augmentation was observed. (F) After implantation on #26 area. (G) After vertical alveolar ridge augmentation using fixture-supported titanium-mesh on #27 area. (H) After removal titanium mesh and secondary surgery of implants, 2mm or more vertical alveolar bone augmentation is observed. (I) Two-years post-surgery, no abnormalities observed.
전신마취 하에 좌측 하악지의 자가골로 block bone을 형성하여 고정한 후, 이종골 이식재 (Bio-Oss® 2g, Geistlich, Seoul, South Korea)로 추가적인 골이식을 시행하였다(Fig. 2C). 비흡수성 차폐막 중 티타늄-메쉬를 이용하여(OssBuilder, Osstem, Seoul, South Korea) 골 이식재를 수복하였으며, Micro screw(Stryker, Michigan, USA) 4mm 3개, 6mm 2개, 8mm 2개를 이용하여 차폐막을 고정하였다.
수술 5개월 후 이식한 자가골 부위의 감염 및 티타늄-메쉬를 고정하였던 Micro screw의 헐거움이 발견되어 감염된 골조직, micro screw 그리고 티타늄-메쉬를 모두 제거하였다. 기존 POMC제거 부위에 임플란트의 초기 고정을 시도할 정도 골은 생성되었지만, 만족할 만한 수직적 치조골 증식이 일어나지는 않았다(Fig. 2D, E).
초기 계획하였던 좌측 상악 구치부 2개의 임플란트 식립보다는, 우선적으로 좌측 상악 제1대구치(#26) 부위의 임플란트 식립 후 경과관찰을 계획하였다. 그 후, 좌측 상악 제1대구치(#26) 부위의 임플란트 고정체(TSIII 4.0 x 11.5mm, Osstem, Seoul, South Korea) 식립을 시행하며, 남은 Micro screw 2개를 제거하였다(Fig. 2F).
임플란트 고정체 식립으로부터 6개월간의 경과관찰 후 좌측 상악 제2대구치(#27) 부위에 임플란트 고정체 지지 형태의 티타늄-메쉬를 이용한 수직적 치조골 증식술을 동반하여 임플란트 고정체(TSIII Mini 3.5 x 10.0mm, Osstem, Seoul, South Korea)를 식립하였다. 이종골 이식재(Bio-Oss ® 0.5g, Geistlich, Seoul, South Korea)를 이용하여 골 이식을 시행한 후 좌측 상악 제1대구치(#26) 부위 및 좌측 상악 제2대구치(#27) 부위의 임플란트 고정체 지지 형태로 티타늄-메쉬 2개를(Ossbuilder, OB2 4[P] x 8[BW] x 7[BL], OB2 10[P] x 12[BW] x 7[BW], Osstem, Seoul, South Korea) 조정하여 이식편의 형태를 잡았다. 조정된 티타늄-메쉬들은 OB anchor screw(3.5 x 0.5mm mini, Osstem, Seoul, South Korea)를 이용하여 각각 좌측 상악 제1대구치(#26) 부위, 좌측 상악 제2대구치(#27) 부위의 임플란트 고정체에 고정되었다(Fig. 2G).
4개월의 치유기간 동안 티타늄-메쉬의 노출은 관찰되지 않았으며, 좌측 상악 제1대구치(#26) 원심부에서 상악 제2대구치(#27) 부위까지 전반적인 3mm 이상의 수직적 치조골 증식이 관찰되었고, 티타늄-메쉬 2개 및 고정용 OB anchor screw 2개는 제거되었다. 동시에 좌측 상악 제1대구치(#26) 및 좌측 상악 제2대구치(#27) 부위의 임플란트에 각각 Healing abutment(4.0 x 5mm, 4.0 x 7mm mini, Osstem, Seoul, South Korea) 체결을 통한 2차수술을 시행하였다(Fig. 2H). 보철적 처치 완료 후 2년 간의 정기적인 경과관찰 결과, 상기 부위 식립된 임플란트는 양호한 골유합과 안정성을 보였다(Fig. 2I).
Case 3
만 24세의 여성 환자가 좌측 상악의 부종 및 불편감을 주소로 내원하였다. 과거력으로 특이병력은 없었다. 임상 검사 및 방사선 검사를 시행하였으며, 함께 시행한 절개 생검 상 Ossifying fibroma 진단되었다(Fig. 3A, B). 전신 마취 하에 외과적 절제술 및 #23, 24, 25, 26, 28의 발치 후 협부 지방이식술을 시행하며, 상악골 형태 유지를 통한 안면 함몰 방지를 위해 좌측 상악골을 철판으로 고정하였다(Fig. 3C, D).
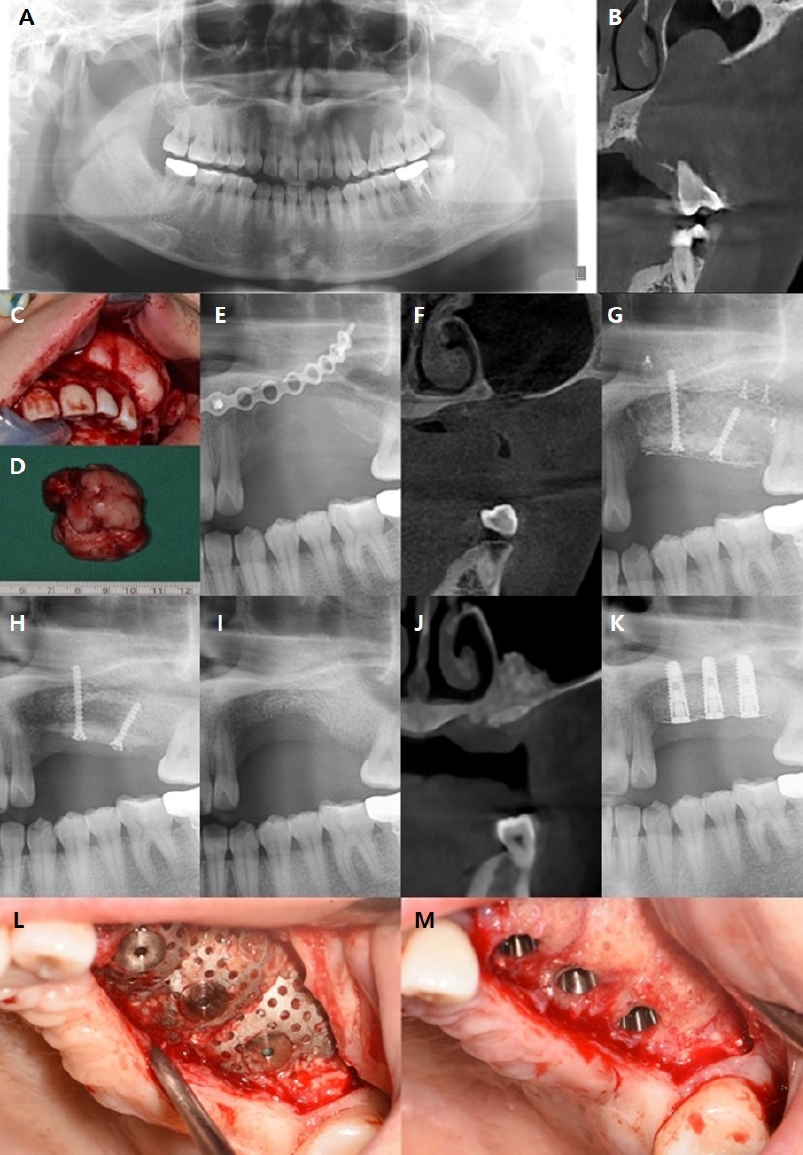
Panoramic radiography (A) & Cone beam computed tomography (B) of the patient taken at the time of first visiting. (C) Clinical photo during surgery. (D) Clinical photo of post-operative mass. Panoramic radiography (E) & Cone beam computed tomography (F) of the patient taken before ramal bone graft, It shows vertical alveolar bone defect. (G) After ramal bone graft surgery with titanium mesh. (H) After removal of titanium mesh and micro screws, additional bone graft was done due to the lack of fusion of bone fragment, but it was unsuccessful. Panoramic radiography (I) & Cone beam computed tomography (J) of the patient taken after bone fragment removed, unsatisfactory alveolar bone augmentation was observed. (K) Five months post-surgery, 3~4mm of vertical alveolar bone augmentation was observed. (L) Clinical photo before titanium mesh removal. (M) Clinical photo after titanium mesh removal, vertical and horizontal alveolar bone augmentation was observed.
2년 6개월의 치유기간 후에 촬영한 해당 부위의 상당한 수직적, 수평적 치조골 결손이 관찰되어, 골이식을 통한 치조골의 수직 및 수평적 증식술을 계획하였다(Fig. 3E, F). 전신마취 하에 좌측 하악지의 자가골로 block bone을 형성하여 고정한 후, 이종골 이식재(Bio-Oss ® 0.5g x 2, Geistlich, Seoul, South Korea)로 추가적인 골이식을 시행하였다. 비흡수성 차폐막 중 티타늄-메쉬를 이용하여(OssBuilder, Osstem, Seoul, South Korea) 골 이식재를 수복하였으며, Micro screw(Stryker, Michigan, USA) 3mm 4개, 10mm 1개, 14mm 1개를 이용하여 차폐막을 고정하였다(Fig. 3G).
수술 6개월 후 티타늄-메쉬 직하방의 골 조각 일부가 유합되지 않아, 티타늄-메쉬와 Micro screw를 제거하였다. 동시에, 합성골 이식재(Frabone ® 0.5g x 2, IB Dental, Seoul, South korea) 와 흡수성 차폐막(OssGuide ® TG-2 20 x 30mm, Osstem, Seoul, South Korea)을 이용하여 추가적인 골이식을 통한 골 유합을 도모하였다(Fig. 3H). 1달의 치유기간 후 골 조각은 여전히 유합되지 않아, 남은 screw와 함께 제거하였다. 자가골 이식부위에 임플란트의 초기 고정을 시도할 정도 골은 생성되었지만, 만족할 만한 수직적 치조골 증식이 일어나지는 않았다(Fig. 3I,J).
4개월간의 경과관찰 후 전신마취 하에 상악 좌측 제1소구치(#24) 부위(TSIII 4.0 x 10.0mm, Osstem, Seoul, South Korea), 상악 좌측 제2소구치(#25) 부위(TSIII 4.0 x 10.0mm, Osstem, Seoul, South Korea), 상악 좌측 제1대구치(#26) 부위(TSIII 4.5 x 10.0mm Osstem, Seoul, South Korea)의 임플란트 고정체를 식립하였다. 이종골 이식재 (Bio-Oss ® 2g, Geistlich, Seoul, South Korea)를 이용하여 골 이식을 시행한 후 임플란트 고정체가 식립된 세 부위에 임플란트 고정체 지지 형태로 티타늄-메쉬 3개를(OssBuilder, Osstem, Seoul, South Korea) 조정하여 이식편의 형태를 잡았다. 조정된 티타늄-메쉬들은 OB anchor screw(Osstem, Seoul, South Korea)를 이용하여 각각 상악 좌측 제1소구치(#24) 부위, 상악 좌측 제2소구치(#25) 부위, 상악 좌측 제1대구치(#26) 부위의 임플란트 고정체에 고정되었다.
5개월의 치유기간 동안 티타늄-메쉬의 노출은 관찰되지 않았고, 상악 좌측 부위의 4~6mm의 수직적 골증식이 확인 되었으며(Fig. 3K), 티타늄-메쉬 3개 및 고정용 OB anchor screw 3개 제거 시행 후 임상적으로 수직 및 수평적 골증식을 확인하였다(Fig. 3L, M). 동시에 상악 좌측 제1소구치(#24) 및 상악 좌측 제2소구치(#25) 부위의 임플란트에 4.0 x 7mm Healing abutment(Osstem, Seoul, South Korea), 상악 좌측 제1대구치(#26) 부위의 임플란트에 4.5 x 7mm의 Healing abutment(Osstem, Seoul, South Korea) 체결을 통한 2차수술을 시행하였다.
Ⅲ. 고찰
임플란트의 장기적으로 안정적인 예후를 위해서 적절한 양과 질의 잔존골이 필수적이다. 골 양을 늘리기 위한 다양한 방법 중에서 골 유도 재생술(Guided Bone Regeneration)은 수직 및 수평 치조골 증식에 모두 적용 가능하며, 필요한 경우 임플란트 식립과 동시에 사용할 수 있는 두 가지 이점이 있어 매우 흔히 사용되는 수술법 중 하나이다[7]. GBR의 성공에는 여러 요인이 영향을 미치며, 차폐막을 사용하지 않았을 때에 비해 적절한 차폐막 사용 시 40% 이상 수직적 골증식 양이 증가한 것으로 미루어 볼 때 차폐막의 역할이 성공적인 GBR에서 중요하다고 할 수 있다[8].
본 연구에서 다룬 티타늄-메쉬는 비흡수성 차폐막으로서 차폐막 하방의 골 이식재에 안정성을 제공하는 우수한 기계적 특성으로 광범위하게 사용되고 있다. 이는 골 이식된 공간을 유지하고, 윤곽의 붕괴를 방지하며, 혈전을 방어하면서도 골 형성 세포만이 골 결손 부위를 다시 채울 수 있도록 충분히 단단하다. 동시에 다루기 쉽고 유연성을 가지며, 크기와 모양의 조절에 용이하다[7]. 또한 치유 과정 동안 형태를 지속적으로 유지하여 하방의 이식재에 대한 압력이나 변위를 방지하며, 최대의 골 증가를 도모한다[9]. 이러한 티타늄-메쉬는 구강악안면외과 영역에서 폭넓게 사용되면서 그 효율성과 안정성은 검증되었다.
그러나 티타늄-메쉬의 단점 중 하나는 다른 차폐막에 비해 치유기간 중 노출의 비율이 높다는 점이다[10]. 평균 노출률은 16.1% 로 보고되며, 노출된 부위에서 약 15%에서 25%의 초기 골 이식편 흡수를 초래하였다[5,11]. 일반적인 티타늄-메쉬는 여러 screw를 사용해서 차폐막을 고정을 해야 하며, 이로 인한 나사 풀림 및 차폐막의 변위를 유발할 수 있다. 또한, 티타늄-메쉬를 적용하기 위하여 다른 차폐막에 비해 더 많은 절개 및 판막의 거상이 요구되며, 이로 인해 술자가 사용에 익숙해지기 까지 많은 시간과 노력이 필요하다.
이러한 기존의 티타늄-메쉬의 단점을 보완하기 위해 최근 기존보다 소형화, 경량화하여 임플란트 고정체에 연결하여 사용하는 방식의 티타늄-메쉬가 사용되고 있다. 이는 기존의 티타늄-메쉬 보다 얇고, 미리 구부려져 있어, 기존의 단점 중 하나인 티타늄-메쉬의 날카로운 면을 줄일 수 있다. 이로 인해, 연조직의 압력을 해소하고, 자극을 줄여 기존의 티타늄-메쉬에 비해 노출을 최소화 할 수 있다[12]. 본 연구에서 사용된 임플란트 고정체 지지 형태의 티타늄-메쉬, 즉, 임플란트 고정체에 cap으로 고정시키는 방법은 다른 종류의 비흡수성 차폐막의 고정에 필요한 기술과 비교했을 때 매우 간단하고 효율적이다. 게다가, 다양한 디자인과 결합된 차폐막의 충분한 강성은 수평 및 수직 결함을 효과적으로 관리할 수 있다[13]. 또 다른 특징은 ‘다공성’ 이며, 이러한 기공은 혈액 공급을 유지하고 세포 외 영양분이 막 전체로 확산되는 데 중요한 역할을 할 수 있어 흡수성 차폐막에 비해 골의 재생을 더욱 촉진한다[14]. 임플란트 고정체 지지 형태의 티타늄-메쉬는 두 가지 다른 기공의 크기를 가지고 있어 골 형성 세포의 이동을 허용하면서 골 이식재의 누출을 차단할 수 있어 효과 적이다[15].
본 연구의 증례 중 두 번째 증례에서 티타늄-메쉬를 이용한 자가골 이식 5개월 후 micro screw의 헐거움으로 티타늄-메쉬와 screw 및 감염된 골조직을 모두 제거했음을 보고하였다. 이는 첫 수술 당시 골 결손 부위가 매우 커 골 이식을 시행한 부위에 대한 차폐막의 완전한 적합성이 떨어졌으며, micro screw 고정력의 부족으로 인한 차폐막의 불안정성이 일차적인 원인으로 생각된다. 또한 일반적인 티타늄-메쉬 사용 시 많은 micro screw 식립으로 인해 screw 부위의 골 재생력 감소, 판막의 과도한 거상으로 인한 술식 시간 증가 및 술식의 복잡성 증가도 예후를 불량하게 만든 것으로 보인다. 세 번째 증례에서는 티타늄-메쉬를 이용한 자가골 이식 6개월 후 차폐막 직하방의 골이 유합되지 않아 제거하였음을 보고하였다. 이는 큰 골 결손 부위로 인해 차폐막의 적합도가 떨어지며 발생한 비골형 연조직 세포의 침입이 영향을 끼친 것으로 보인다. 또한, 차폐막이 혈액공급을 방해하거나 부분적으로 차단할 경우 골 유도 재생을 방해할 수 있다[16]. 티타늄-메쉬를 이용할 때 중요한 것은 차폐막의 고정으로, 차폐막의 고정에 문제가 생김과 함께 다양한 요인들이 두 증례 모두에서 첫 번째 골 이식 시 발생한 골재생의 부족에 영향을 미쳤음을 알 수 있다. 두 증례 모두 비록 첫 번째 골이식에 만족스러운 결과를 도출해 내지는 못했지만, 임플란트 식립을 통한 초기 고정을 기대할 수 있을 정도로의 수직적 골 증식은 이루어 내었다. 이러한 경우에 차폐막의 고정에 보다 유리한 임플란트 고정체 지지 형태의 티타늄-메쉬를 이용한 골 이식이 차선책으로 선택될 수 있으며, 본 연구는 이를 통해 예지성 있는 결과를 보였으므로 이에 보고하는 바이다.
임플란트 고정체 지지 형태의 티타늄-메쉬를 활용한 골증식술은 기존 티타늄 메쉬의 장단점을 고려하여 진행된다. 기존 티타늄-메쉬의 장점 중 안정성, 강성, 그리고 다양한 크기와 모양에 대한 유연성은 골증식에 있어서 중요한 특성으로 간주된다[17]. 그러나 동시에, 노출의 위험성과 초기 골이식 흡수에 대한 우려가 존재한다. 임플란트 고정체 지지 방법은 노출 위험성을 낮추는 데에 기여하며, 초기 골이식 흡수에 미치는 영향을 최소화하고 차폐막의 고정에 보다 유리하다. 이러한 특징들은 임플란트 고정체 지지 형태의 티타늄-메쉬가 기존 티타늄 메쉬의 한계를 극복하고, 골이식 수술의 효율성과 안전성을 향상시킬 수 있다는 잠재력을 제시한다. 따라서, 임플란트 고정체 지지 티타늄-메쉬는 기존의 티타늄-메쉬의 장점을 유지하면서도 새로운 골이식 기술의 발전과 안정성을 모색하는 데에 효과적인 해결책으로 여겨질 수 있다. 이러한 고찰을 통해 임플란트 고정체 지지 형태의 티타늄-메쉬가 골 증식술에서의 임상적인 어려움을 극복하고, 환자에게 더 나은 임상 결과를 제공할 수 있을 것으로 기대된다.
Ⅳ. 결론
위 증례들은 임플란트 고정체 지지 티타늄-메쉬 차폐막을 이용한 골이식을 시행하여 치조골을 수직 및 수평적으로 증식시켰다. 티타늄-메쉬는 연조직의 붕괴를 방지할 충분한 견고성을 갖추고 있으며, 골 이식 부위의 공간을 유지하면서도 연성이 뛰어나고 조작성이 좋다. 또한, 공간 형성 능력이 뛰어나 윤곽을 만들고, 골 결손부위에 맞게 조정할 수 있었다. 하지만, 여러 screw를 사용해서 고정을 해야하며, 치유과정 중 노출이 발생하기도 한다. 위 단점을 보완하기 위해 본 연구에서는 일차적으로 시행한 골이식이 실패한 상황에서도 임플란트를 식립과 동시에 임플란트 고정체 지지 형태의 티타늄-메쉬를 이용하여 성공적으로 치조골의 수직적 높이를 증식시켰으므로, 이에 보고하는 바이다.
임플란트 고정체 지지 형태의 티타늄-메쉬 차폐막은 치조골의 수직적 증식술에 보다 효과적으로 사용될 수 있으며, 기존의 티타늄-메쉬가 갖는 단점을 최소화하기 위한 연구 및 개선이 지속적으로 필요할 것이다.
V. 이해상충(Conflicts of Interest)
Patient treated with titanium-mesh assisted vertical alveolar bone augmentation