Necessity of Anatomy Education for Dental School Students Utilizing 3D and Virtual Reality Technologies: A Narrative Review
Article information

Abstract
Members of dental academia are eager to embrace innovative tools for anatomy education. The proliferation of technological resources has facilitated the integration of virtual systems into dental and medical education. This is considered paramount for communicating the anatomical knowledge essential for safe and competent medical practice. Among these tools, three-dimensional (3D) anatomy models, virtual reality (VR) simulations, and haptic technologies are pivotal for educating students and training healthcare professionals. This narrative review discusses these topics based on published outcomes from the past decade, emphasizing their potential in anatomical learning and clinical practice, particularly during the COVID-19 pandemic. Substantial interest and positive impacts have been reported by educators and students regarding the utilization of 3D VR. 3D VR enables precise and high-resolution representations of organ structure, vascular formation, and nerve distribution. It enriches anatomical, clinical, and radiological learning and familiarizes individuals with the anatomical and radiological features of real patients. Furthermore, 3D VR ensures the continuity of anatomical and surgical training through online platforms, making the strategic deployment of these devices especially pertinent during quarantine. Therefore, dental education and clinical applications using 3D VR, augmented reality, and haptic technology are expected to become an unstoppable trend.
Ⅰ. Introduction
Virtual reality (VR) simulations have recently been introduced in dental education as an adjunct to traditional curricula to train dental students before they interact with real patients. Dental education differs from other forms of medical education because it combines theoretical knowledge, laboratory findings, and clinical practice [1]. Difficulties in dental education stem from the fact that the acquisition of theoretical knowledge requires spatial imagination, and patient-centered education using traditional mannequin simulations does not resemble realistic clinical situations [2]. Preclinical and clinical training are paramount for developing fine motor skills to prepare dental students to participate in the dental profession [3]. Many required dental education competency skills are difficult to acquire and require repeated training and extensive practice. Since the outbreak of the novel coronavirus SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) in December 2019, all essential human activities have been affected by social distancing measures [4], and education in the field of dentistry has also been affected. A one-to-one dental education model is necessary in dental education, but this design had to be partially replaced by digital or virtual settings to avoid gathering teenagers or young adults in closed spaces.
VR is recognized as a valuable tool for teaching dental students. Recently, the use of VR in dental schools has increased worldwide. VR is defined as a computer-generated medical simulation of a three-dimensional (3D) image or environment using software to create an immersive computer-generated environment [5]. Users of three-dimensional VR (3D VR) simulation technology can wear a head-mounted display device, which provides an experience that allows them to engage with settings and virtual characters in a manner that feels real [6]. VR can be beneficial in dental education by allowing for a non-contact learning environment emulating the patients. VR is combined with many other cutting-edge technologies and has high potential for use in education in the fields of dentistry and anatomy.
Augmented reality (AR) is a type of computer-generated graphics that is superimposed on real-world scenes. AR differs from VR because it does not reproduce natural conditions [7]. AR refers to a technology that integrates real and virtual elements into a combined experience and allows learners to visualize complex spatial relationships, abstract concepts, and experiential phenomena that are not possible in the real world, especially in surgical coaching [8,9]. Immersive virtual reality is a form of AR in which users interact with digital 3D environments recreated through 360-degree real-world recordings [10].
Haptic technology is a modern simulation method that involves tactile sensation while interacting with computer-generated objects [11]. The concept of haptic education was introduced approximately ten years ago 12. Haptics refers to the sense of touch and consists of the science that integrates interaction with the external environment through touch [13]. By implementing these technologies in dental education, designers can be motivated to create virtual teeth, gingiva, alveolar bone, and oral mucosa with or without pathological damage or to indicate by vibration the presence or absence of pain when palpating the temporomandibular joint (TMJ) and/or masticatory muscles. To increase realism, we can create multilayered virtual anatomical structures, including teeth, TMJs, and facial muscles, with varying mechanical characteristics [14].
The application of VR in dental education has attracted the attention of researchers even during the early experimental stages. It has been suggested that this could be expanded to include the preparation of teeth for prosthetic treatment, endodontics, and orthodontic treatment and could improve dental education compared with traditional education, particularly in restorative dentistry and dental surgery training [15,16]. Although no actual research has been conducted, there is a good possibility that it can be used for examination of the TMJ or masticatory muscles, as well as for clinical examination of temporomandibular disorders (TMDs). VR has enabled remote online course delivery possible through 3D VR workshops [17]. The flexibility of the technology allows attendees to contribute actively [18,19]. Despite technical limitations, a 3D VR understanding of the surgery and associated anatomy was facilitated 20. However, its effectiveness in dental education remains controversial. Therefore, this narrative review aimed to introduce and evaluate the application and effectiveness of VR simulations in dental education.
Ⅱ. Materials and Methods
Data were systematically gathered and compiled from various databases including PubMed, Scopus, and Google Scholar, focusing on articles and reviews published within the past decade. The key search terms employed included anatomy, human anatomy, virtual reality, augmented reality, three-dimensional, education, dental and dental procedures, implant surgery, TMJ, TMD, anatomy teaching, haptic technology, COVID-19, and e-learning. A total of 71 articles meeting the specified criteria were selected and included in this review. This systematic review was conducted using the Scale for the Assessment of Narrative Review Articles (SANRA), a brief critical appraisal tool for the assessment of non-systematic articles [21]. Only studies with a score of 6 or higher based on SANRA (Scale for the Assessment of Narrative Review Articles) were included in this narrative review. The results are organized into three distinct sections.
Ⅲ. Results
1. Advantages and limitations of anatomy education using 3D VR
3D anatomy and virtual dissection tools have become integral components of gross anatomy courses in dental and medical schools, with numerous authors highlighting their positive impacts on student learning [22]. The success of these tools is so pronounced that they have the potential to replace traditional cadaveric dissections in certain procedures. Studies have demonstrated the equivalence of studying the musculoskeletal system of the entire human body through 3D anatomy and virtual dissection tools compared to cadaveric dissection [23,24]. These tools are not only engaging but also highly effective as educational aids, particularly for students who leverage technology in their learning processes. Dental and medical students expressed enthusiasm for studying male and female gross anatomy, categorized by race and sex, using life-size touchscreen tables with virtual human cadavers [25]. The interactive platform allows students to dissect, rotate, and magnify anatomical features, providing the capability to isolate and focus on individual organs by eliminating the associated structures [26]. Filters can be used to analyze specific structures, such as blood vessels or nerves, and particular anatomical regions. Users can highlight vessels or nerves in different colors, and annotation features can aid in identification [27].
Although the 3D VR human body provides a comprehensive vascularization representation, further improvements are needed to accurately depict and highlight nerve branches. Despite the advantages of 3D anatomy and virtual dissection tools for students, the need for the ability to dissect digital human cadavers virtually, understand organ deformations, and recognize anatomical variations has been emphasized [28]. This tool is especially valuable for educating dental and medical students about variations that may not be immediately apparent in cadavers with oral or systemic diseases. The programming capabilities of these tools enable simulation of tissue deformation caused by diseases, emphasizing specific anatomical areas for identification. Additionally, the diverse distribution of nerves, blood vessels, muscles, and bone joints in the facial area underscores the importance of developers addressing both normal and rare variations or natural changes from aging in anatomical structures [29]. Attention to detail is crucial for enhancing students’ and clinicians’ understanding of 3D anatomy and virtual dissection tools.
2. Dental education and clinical application of 3D VR
Currently, a variety of computer-based 3D application tools are becoming regular tools for dental students in education and self-learning, and cutting-edge VR- and AR-based technologies are recognized as next-generation dental education tools. AR and VR need to be equipped with head and neck anatomy, and the use of AR provides an additional means of training dental anatomy compared with traditional modes [30]. In a study on teaching dental morphologies to preclinical students using VR, 34.9% stated that they understood dental morphologies much better, 57.1% better, and 7.9% equally well compared to using a traditional textbook [31]. Manual dexterity training was conducted in first-year dental students, and 3D vision had a better learning effect than students who worked in 2D [32]. When VR is used by senior dental students, it has the potential to improve basic dental diagnostic skills and can be used as an auxiliary educational tool [33]. In restorative dentistry, including cavity preparations and filling material applications, students’ manual skills have significantly improved with haptic technologies such as VR, VR simulators, and interactive video games [34~36]. By immersing cone-beam computed tomography (CT) in VR, dental students can understand the maxillofacial area and effectively learn head and neck anatomy from a more three-dimensional and multifaceted perspective [37]. For each task in a dental treatment procedure, the learning effect can be improved through haptic feedback [38]. Surgical training programs that can be applied to dental students or clinicians are being developed after each stage of implant surgery and implemented in 3D VR [39]. Approximately 80% of students reported their 3D VR learning experience enjoyable, indicating a preference for in-person VR over online VR [40]. The knowledge gained in this manner is important for evaluating and diagnosing many benign and malignant conditions of the head and neck region. Practicing maxillofacial surgery with computerized virtual patients can improve short- and long-term learning efficiency, self-assessed competence, and student satisfaction [41]. In the training of implant surgery, haptic simulators can provide practical advantages in implant surgery training [42]. Learning using 360° videos was significantly more effective in acquiring dental radiology knowledge than dental radiology education through traditional textbooks [43]. More attention has been paid to the long-term effects and implications of these technologies and educational techniques. Furthermore, in most dental practices, when education must be conducted non-face-to-face or when it is impossible to proceed or participate in practice because of school or student circumstances, a new educational tool is needed to provide indirect experience and enable knowledge acquisition.
3. Diagnosis and treatment of patients with TMD using 3D VR
The application of 3D VR for the examination of the TMJ and surrounding masticatory muscles has been scarce in existing studies. Nevertheless, a comparative analysis revealed no statistically significant difference in the surgical success rates between CT-guided and 3D VR-guided TMJ arthroplasty for cases involving ankylosis of the TMJ [44]. Integrating haptic technology with 3D VR technology holds promise for palpation tests conducted during the clinical diagnosis of TMDs, particularly for assessing TMJ and muscle areas. This integration allows positive vibration stimulation when the learner or clinician places their hand or finger on the relevant anatomical test site. Furthermore, introducing a virtual TMD patient case into a 3D VR tool enables a computer entity to respond actively to palpation tests conducted by the surgeon. Consequently, 3D VR is expected to be highly beneficial for TMD diagnosis, treatment, and post-treatment monitoring. Efforts to immerse magnetic resonance imaging (MRI) into 3D VR formats are being attempted, albeit minimally [45], and are expected to be useful for observing the TMJ and diagnosing TMD. Eight weeks of extremity muscle-strengthening training using VR was effective in adolescents with intellectual disability [46]. The VR training program improved the sense of balance in elderly people in a daily program at a nursing home, proving its potential as a treatment strategy [47]. VR-based exercises are effective for reducing functional limitations in patients with chronic neck pain [48]. Utilizing VR with body movements as an interactive interface with a computer represents a novel approach for treatment in rehabilitation settings. VR treatment has noteworthy effects in reducing pain, increasing joint mobility, and enhancing functional capacity in patients with chronic musculoskeletal pain [49]. Therefore, the use of VR in both myogenous TMD, including myalgia or myofascial pain, and arthrogenous TMD, including arthralgia and degenerative joint diseases, has the potential to be helpful for treatment.
Ⅳ. Discussion
Dental education and clinical applications of 3D VR, AR, and haptic technology are expected to become unstoppable trends. Recent studies have recommended 3D VR-based dental education for students. In particular, using VR human bodies is helpful when studying not only dental anatomy but also whole body anatomy [50]. In addition, the use of this virtual human body is attractive when universities do not have access to cadavers for anatomical practice. This tool allows students to dissect lifesized digital human cadavers and understand organ deformation [51]. Knowing anatomical variations is very important in the education or training of various oral diseases and in diagnosing the pain status of dental students and clinicians. Perhaps a program integrated into the device could be used to easily detect abnormal or disease-related deformations in a cadaver compared to normal anatomy. The accumulation of traditional anatomical knowledge is important for students' discovery of anatomical variations [52]. Progressive work is required to add new patient cases or scenarios to the VR tool, which will be useful for students and clinicians in responding to unexpected situations and preventing injuries during procedures or surgeries in humans.
Traditionally, dental and medical education consists of theoretical learning in the classroom and clinical training in dental hospitals, where students gain clinical experience [53]. This is primarily conducted through face-to-face education between professors and students. However, there has recently been a shift toward greater adoption of technology in dental education. This was further accelerated by the COVID-19 pandemic, which began in December 2019 [54], and continues to affect dental education. As it has become clear that social distancing has reduced the spread of COVID-19, educators have had to reconsider how best to teach students while reducing the number of in-person classes. To solve these problems, various digital education tools such as e-learning, 3D VR programs, and VR simulators have emerged [55]. In addition, in the field of dentistry, these tools and technologies have been expanded not only for student education but also for clinician training with good results, as mentioned earlier.
Certain pedagogical practices are indispensable to achieve a comprehensive understanding of anatomy. Human anatomy plays a distinctive and vital role in dental education, making it impractical to suspend such education even during prolonged pandemics. VR technology has emerged as a viable alternative for teaching essential subjects such as histology, anatomy, and physiology within the dental curriculum [56,57]. VR tools and technologies can serve as valuable resources allowing students to learn about the intricacies of oral and gross anatomy through online platforms, particularly during a pandemic [58]. Face-to-face education is important in dental education; however, the experience of using non-face-to-face education, e-learning, and various technologies during the pandemic was very positive for both students and professors. Therefore, it is highly likely that these new educational methods or auxiliary tools will become incorporated into traditional educational methods in the future.
The COVID-19 pandemic is nearing an end in January 2024. However, the integration of VR in anatomy education remains pertinent. Large-scale, multilayered VR human bodies can be deployed across education and practice sites [6,59], enhancing the effectiveness of teaching anatomy and fundamental dentistry concepts. This is particularly relevant because VR human bodies can be seamlessly integrated with software such as Touch Surgery, which is compatible with tablets or smartphones [60,61]. This integration enables the continuation of various dental procedures and surgical training. The potential of VR technologies to fulfill the learning objectives of both students and clinicians continues to grow, signifying their enduring relevance to dental education.
The application of 3D VR in dental education has strengths and limitations, as illustrated in Figure 1. One of the primary advantages of 3D VR is the immersive and interactive learning experience it provides, capturing student attention and fostering engagement [62]. VR facilitates hands-on learning within a simulated environment, promoting practical understanding of intricate dental concepts. In addition, virtual environments empower students to explore locations and scenarios that may be inaccessible in the real world, thereby broadening the scope of educational experiences [63]. Furthermore, VR allows customization of individual learning styles, delivery of tailored educational content, and pacing. In dental or hazardous environments, VR establishes a secure and controlled setting for training without real-world risks [64].
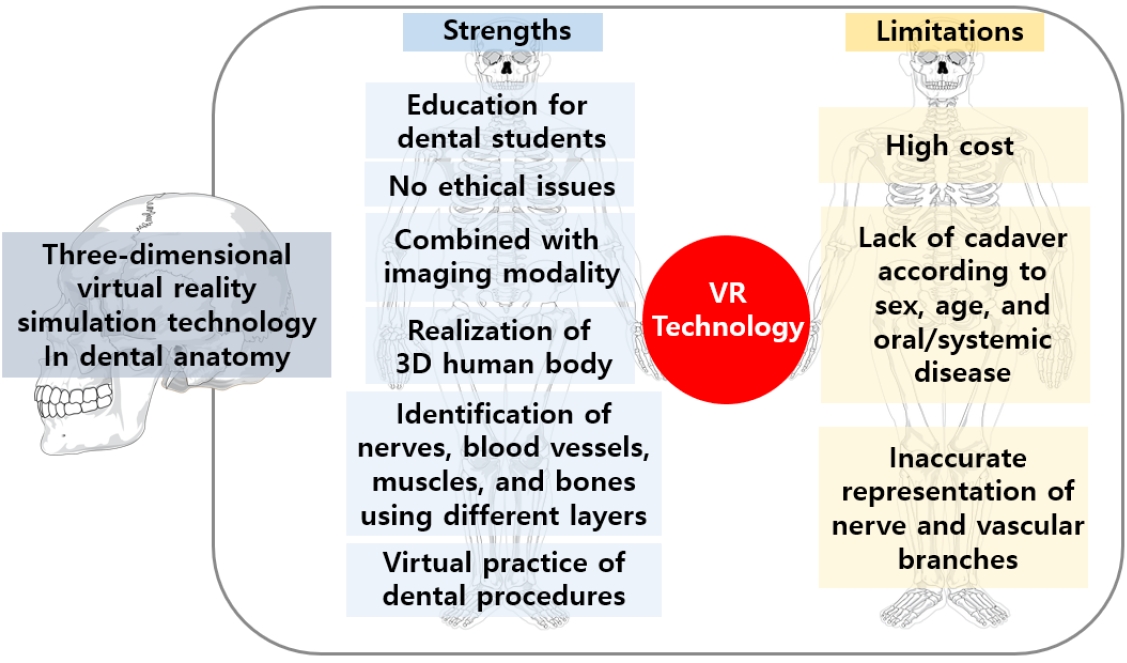
Strengths and limitations when applying 3D VR to dental anatomy and education
Employing VR and realism in education can be a two-sided coin. There are notable limitations to the use of VR in dental education. The implementation of VR technology can incur substantial costs, including both initial setup expenses and ongoing maintenance [65]. However, some argue that 3D VR is ultimately cost-effective because it makes education more accessible, aligns with student preferences, and does not incur significant additional costs [40]. Technical challenges arise because VR systems require specialized equipment and expertise, posing difficulties for schools or institutions with limited resources [66]. The extended use of VR may engender a sense of isolation among students as they become immersed in a virtual world rather than interacting with their real-world surroundings or peers [67]. Moreover, prolonged exposure to VR may cause discomfort or health issues including eye strain, motion sickness, and other potential side effects [68]. Although VR content is expanding, there may still be limitations in the availability of high-quality educational materials for certain dental subjects [69]. VR technology encounters various ethical dilemmas, such as diminished user autonomy, health risks, and privacy concerns [70]. As the need for digital learning to supplant physical and visual experiences grows, 3D VR is emerging as a valuable tool for crafting educational virtual environments. While lifelike simulations may enhance comprehension in certain dental subjects, they may impede understanding in others. Therefore, while VR enhances specific aspects of dental education, a thorough assessment of its costs, technical prerequisites, and potential drawbacks is imperative for its effective implementation. It is certain that the introduction of these technologies into dentistry will become an unstoppable trend, and we must actively consider, research, develop, and implement this trend in a practical way.
Ⅴ. Conclusion
3D VR, by emulating the real world, is poised for widespread implementation across diverse domains of preclinical training for dental students. This includes applications in dental education, training of surgical skills, and the diagnosis and treatment of diseases. There is growing recognition of the importance of improved teaching technology in the success of preclinical education [71]. When students receiving training do not receive realistic feedback in a timely manner, their learning efficiency is low and their training effectiveness is poor. Therefore, cutting-edge 3D VR, which has proven usefulness and has explosive potential, is worth utilizing in education in each field of dentistry.
Ⅵ. Competing interests:
The author declares no competing interests.
Notes
AUTHOR CONTRIBUTIONS
Y.-H.L. wroyr manuscript and prepared the original draft. Conceptualization, Methodology, Software, Validation, Formal analysis, Investigation, Resources, Data curation, Writing-review and editing, Visuakization, Supervision, Project administration, Funding acquistion.
DATA AVAILABILITY STATEMENT
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
ETHICS DECLARATION
The review of the protocol of this study was waived by the Institutional Review Board of Kyung Hee University Dental Hospital in Seoul, South Korea.
Funding
This work was supported by the Korea Medical Device Development Fund grant funded by the Korean government (Ministry of Science and ICT, Ministry of Trade, Industry, and Energy, Ministry of Health & Welfare, Republic of Korea, Ministry of Food and Drug Safety) (Project Number: KMDF_PR_20200901_0023, 9991006696).